
Page 41 - World Journal of Laparoscopic Surgery
P. 41
Role of NOTES in the Diagnosis of Women Pelvic Pathologies
Contd... retrieval procedures carry a risk of infection, which is estimated
at 0.4%, whether or not vaginal disinfection is performed (Dicker
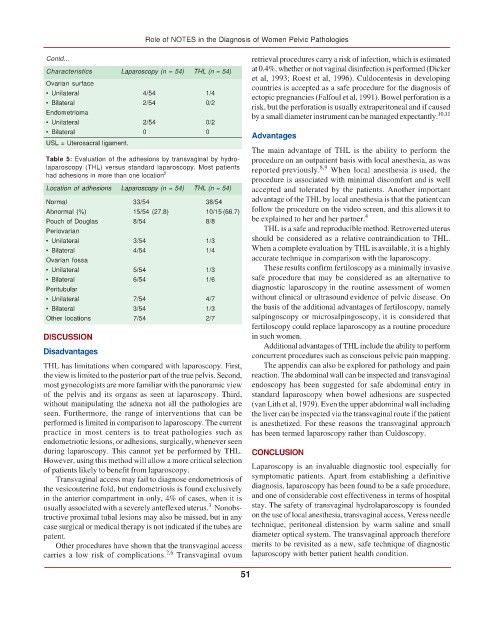
Characteristics Laparoscopy (n = 54) THL (n = 54)
et al, 1993; Roest et al, 1996). Culdocentesis in developing
Ovarian surface countries is accepted as a safe procedure for the diagnosis of
• Unilateral 4/54 1/4 ectopic pregnancies (Falfoul et al, 1991). Bowel perforation is a
• Bilateral 2/54 0/2 risk, but the perforation is usually extraperitoneal and if caused
Endometrioma by a small diameter instrument can be managed expectantly. 10,11
• Unilateral 2/54 0/2
• Bilateral 0 0
Advantages
USL = Uterosacral ligament.
The main advantage of THL is the ability to perform the
Table 5: Evaluation of the adhesions by transvaginal by hydro- procedure on an outpatient basis with local anesthesia, as was
laparoscopy (THL) versus standard laparoscopy. Most patients reported previously. When local anesthesia is used, the
8,9
had adhesions in more than one location 2
procedure is associated with minimal discomfort and is well
Location of adhesions Laparoscopy (n = 54) THL (n = 54) accepted and tolerated by the patients. Another important
Normal 33/54 38/54 advantage of the THL by local anesthesia is that the patientcan
Abnormal (%) 15/54 (27.8) 10/15 (66.7) follow the procedure on the video screen, and this allows it to
4
Pouch of Douglas 8/54 8/8 be explained to her and her partner.
Periovarian THL is a safe and reproducible method. Retroverted uterus
• Unilateral 3/54 1/3 should be considered as a relative contraindication to THL.
• Bilateral 4/54 1/4 When a complete evaluation by THL isavailable, it is a highly
Ovarian fossa accurate technique in comparison with the laparoscopy.
• Unilateral 5/54 1/3 Theseresults confirm fertiloscopy as a minimally invasive
• Bilateral 6/54 1/6 safe procedure that may be considered as an alternative to
Peritubular diagnostic laparoscopy in the routine assessment of women
• Unilateral 7/54 4/7 without clinical or ultrasound evidence of pelvic disease. On
• Bilateral 3/54 1/3 the basis of the additional advantages of fertiloscopy, namely
Other locations 7/54 2/7 salpingoscopy or microsalpingoscopy, it is considered that
fertiloscopy could replace laparoscopy as a routine procedure
DISCUSSION in such women.
Additional advantages of THL include the ability to perform
Disadvantages
concurrent procedures such as conscious pelvic pain mapping.
THL has limitations when compared with laparoscopy. First, The appendix can also be explored for pathology and pain
theview is limited to the posterior part of the true pelvis. Second, reaction. The abdominal wall can be inspected and transvaginal
most gynecologists are more familiar with the panoramic view endoscopy has been suggested for safe abdominal entry in
of the pelvis and its organs as seen at laparoscopy. Third, standard laparoscopy when bowel adhesions are suspected
without manipulating the adnexa not all the pathologies are (van Lith et al, 1979). Even the upper abdominal wall including
seen. Furthermore, the range of interventions that can be the liver can be inspected via the transvaginal route if the patient
performed is limited in comparisonto laparoscopy. The current is anesthetized. For these reasons the transvaginal approach
practice in most centers is to treat pathologies such as has been termed laparoscopy rather than Culdoscopy.
endometriotic lesions, or adhesions, surgically,whenever seen
during laparoscopy. This cannot yet be performed by THL. CONCLUSION
However, using this method will allow a more criticalselection
of patients likely to benefit from laparoscopy. Laparoscopy is an invaluable diagnostic tool especially for
Transvaginal access may fail to diagnose endometriosis of symptomatic patients. Apart from establishing a definitive
the vesicouterine fold, but endometriosis is found exclusively diagnosis, laparoscopy has been found to be a safe procedure,
in the anterior compartment in only, 4% of cases, when it is and one of considerable cost effectiveness in terms of hospital
3
usually associated with a severely anteflexed uterus. Nonobs- stay. The safety of transvaginal hydrolaparoscopy is founded
tructive proximal tubal lesions may also be missed, but in any on the use of local anesthesia, transvaginal access, Veress needle
case surgical or medical therapy is not indicated if the tubes are technique, peritoneal distension by warm saline and small
patent. diameter optical system. The transvaginal approach therefore
Other procedures have shown that the transvaginal access merits to be revisited as a new, safe technique of diagnostic
2,6
carries a low risk of complications. Transvaginal ovum laparoscopy with better patient health condition.
51