
Page 27 - WJOLS - Laparoscopic Journal
P. 27
Fadare Oluwaseun O
7
and Margalioth reviewed 90 articles, reporting on a total of Over time, a variety of classifications of the syndrome
2981 cases of Asherman’s syndrome in various countries; have been based on different diagnostic tools. According to
they found that the incidence was especially high in Israel their findings on hysterosalpingography (HSG), Toaff and
9
(25.8%), Greece (15.3%) and South America (14.9%). The Ballas classified intrauterine adhesions into four groups,
prevalence of adhesions varied geographically, and the based on a semiquantitative evaluation. With the advent of
discrepancies could be explained by several factors: hysteroscopy, various investigators have created a series
1. The degree of awareness of the clinicians. of classifications 10-12 based on the extent of adhesions and
2. The number of therapeutic and illegal abortions in the visualization of the ostia. However, none of these
different parts of the world. classifications took into account the various clinical
3. the kind of instrument used for puerperal and postabortal presentations, especially with regard to the menstrual history.
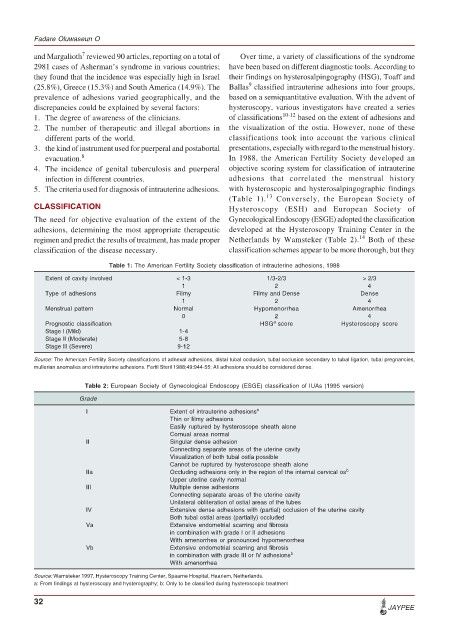
evacuation. 8 In 1988, the American Fertility Society developed an
4. The incidence of genital tuberculosis and puerperal objective scoring system for classification of intrauterine
infection in different countries. adhesions that correlated the menstrual history
5. The criteria used for diagnosis of intrauterine adhesions. with hysteroscopic and hysterosalpingographic findings
13
(Table 1). Conversely, the European Society of
CLASSIFICATION Hysteroscopy (ESH) and European Society of
The need for objective evaluation of the extent of the Gynecological Endoscopy (ESGE) adopted the classification
adhesions, determining the most appropriate therapeutic developed at the Hysteroscopy Training Center in the
14
regimen and predict the results of treatment, has made proper Netherlands by Wamsteker (Table 2). Both of these
classification of the disease necessary. classification schemes appear to be more thorough, but they
Table 1: The American Fertility Society classification of intrauterine adhesions, 1988
Extent of cavity involved < 1-3 1/3-2/3 > 2/3
1 2 4
Type of adhesions Filmy Filmy and Dense Dense
1 2 4
Menstrual pattern Normal Hypomenorrhea Amenorrhea
0 2 4
a
Prognostic classification HSG score Hysteroscopy score
Stage l (Mild) 1-4
Stage ll (Moderate) 5-8
Stage lll (Severe) 9-12
Source: The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies,
mullerian anomalies and intrauterine adhesions. Fertil Steril 1988;49:944-55: All adhesions should be considered dense.
Table 2: European Society of Gynecological Endoscopy (ESGE) classification of IUAs (1995 version)
Grade
I Extent of intrauterine adhesions a
Thin or filmy adhesions
Easily ruptured by hysteroscope sheath alone
Cornual areas normal
II Singular dense adhesion
Connecting separate areas of the uterine cavity
Visualization of both tubal ostia possible
Cannot be ruptured by hysteroscope sheath alone
IIa Occluding adhesions only in the region of the internal cervical os b
Upper uterine cavity normal
III Multiple dense adhesions
Connecting separate areas of the uterine cavity
Unilateral obliteration of ostial areas of the tubes
IV Extensive dense adhesions with (partial) occlusion of the uterine cavity
Both tubal ostial areas (partially) occluded
Va Extensive endometrial scarring and fibrosis
in combination with grade I or II adhesions
With amenorrhea or pronounced hypomenorrhea
Vb Extensive endometrial scarring and fibrosis
in combination with grade III or IV adhesions b
With amenorrhea
Source: Wamsteker 1997, Hysteroscopy Training Center, Spaarne Hospital, Haarlem, Netherlands.
a: From findings at hysteroscopy and hysterography; b: Only to be classified during hysteroscopic treatment
32
JAYPEE