
Page 17 - WJOLS - Laparoscopic Journal
P. 17
Aryan Ahmed
not used routinely, a significant number of therapeutic double the risk in a compromised unstable patient, this is a
procedures were applied like repair of injured diaphragm question that has been answered by many pioneers of trauma
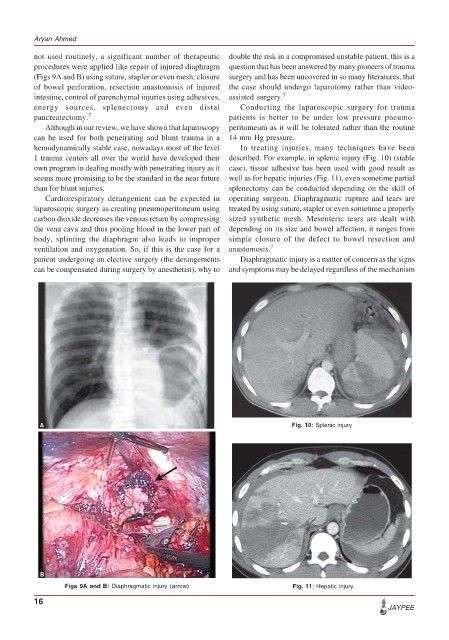
(Figs 9A and B) using suture, stapler or even mesh, closure surgery and has been uncovered in so many literatures, that
of bowel perforation, resection anastomosis of injured the case should undergo laparotomy rather than video-
intestine, control of parenchymal injuries using adhesives, assisted surgery. 5
energy sources, splenectomy and even distal Conducting the laparoscopic surgery for trauma
pancreatectomy. 7 patients is better to be under low pressure pneumo-
Although in our review, we have shown that laparoscopy peritomeum as it will be tolerated rather than the routine
can be used for both penetrating and blunt trauma in a 14 mm Hg pressure.
hemodynamically stable case, nowadays most of the level In treating injuries, many techniques have been
1 trauma centers all over the world have developed their described. For example, in splenic injury (Fig. 10) (stable
own program in dealing mostly with penetrating injury as it case), tissue adhesive has been used with good result as
seems more promising to be the standard in the near future well as for hepatic injuries (Fig. 11), even sometime partial
than for blunt injuries. splenectomy can be conducted depending on the skill of
Cardiorespiratory derangement can be expected in operating surgeon. Diaphragmatic rupture and tears are
laparoscopic surgery as creating pneumoperitoneum using treated by using suture, stapler or even sometime a properly
carbon dioxide decreases the venous return by compressing sized synthetic mesh. Mesenteric tears are dealt with
the vena cava and thus pooling blood in the lower part of depending on its size and bowel affection, it ranges from
body, splinting the diaphragm also leads to improper simple closure of the defect to bowel resection and
ventilation and oxygenation. So, if this is the case for a anastomosis. 7
patient undergoing an elective surgery (the derangements Diaphragmatic injury is a matter of concern as the signs
can be compensated during surgery by anesthetist), why to and symptoms may be delayed regardless of the mechanism
A Fig. 10: Splenic injury
B
Figs 9A and B: Diaphragmatic injury (arrow) Fig. 11: Hepatic injury
16
JAYPEE