
Page 50 - Journal of WALS
P. 50
WJOLS
Mayer-Rokitansky-Kuster-Hauser Syndrome
contd...
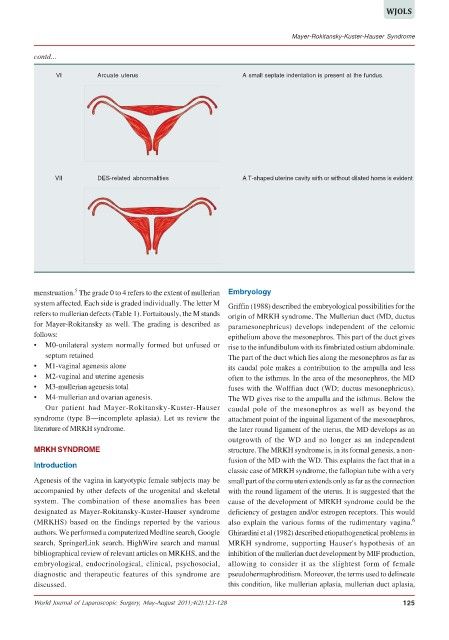
VI Arcuate uterus A small septate indentation is present at the fundus.
VII DES-related abnormalities A T-shaped uterine cavity with or without dilated horns is evident
5
menstruation. The grade 0 to 4 refers to the extent of mullerian Embryology
system affected. Each side is graded individually. The letter M Griffin (1988) described the embryological possibilities for the
refers to mullerian defects (Table 1). Fortuitously, the M stands origin of MRKH syndrome. The Mullerian duct (MD, ductus
for Mayer-Rokitansky as well. The grading is described as paramesonephricus) develops independent of the celomic
follows: epithelium above the mesonephros. This part of the duct gives
• M0-unilateral system normally formed but unfused or rise to the infundibulum with its fimbriated ostium abdominale.
septum retained The part of the duct which lies along the mesonephros as far as
• M1-vaginal agenesis alone its caudal pole makes a contribution to the ampulla and less
• M2-vaginal and uterine agenesis often to the isthmus. In the area of the mesonephros, the MD
• M3-mullerian agenesis total fuses with the Wolffian duct (WD; ductus mesonephricus).
• M4-mullerian and ovarian agenesis. The WD gives rise to the ampulla and the isthmus. Below the
Our patient had Mayer-Rokitansky-Kuster-Hauser caudal pole of the mesonephros as well as beyond the
syndrome (type B—incomplete aplasia). Let us review the attachment point of the inguinal ligament of the mesonephros,
literature of MRKH syndrome. the later round ligament of the uterus, the MD develops as an
outgrowth of the WD and no longer as an independent
MRKH SYNDROME structure. The MRKH syndrome is, in its formal genesis, a non-
fusion of the MD with the WD. This explains the fact that in a
Introduction
classic case of MRKH syndrome, the fallopian tube with a very
Agenesis of the vagina in karyotypic female subjects may be small part of the cornu uteri extends only as far as the connection
accompanied by other defects of the urogenital and skeletal with the round ligament of the uterus. It is suggested that the
system. The combination of these anomalies has been cause of the development of MRKH syndrome could be the
designated as Mayer-Rokitansky-Kuster-Hauser syndrome deficiency of gestagen and/or estrogen receptors. This would
(MRKHS) based on the findings reported by the various also explain the various forms of the rudimentary vagina. 6
authors. We performed a computerized Medline search, Google Ghirardini et al (1982) described etiopathogenetical problems in
search, SpringerLink search, HighWire search and manual MRKH syndrome, supporting Hauser's hypothesis of an
bibliographical review of relevant articles on MRKHS, and the inhibition of the mullerian duct development by MIF production,
embryological, endocrinological, clinical, psychosocial, allowing to consider it as the slightest form of female
diagnostic and therapeutic features of this syndrome are pseudohermaphroditism. Moreover, the terms used to delineate
discussed. this condition, like mullerian aplasia, mullerian duct aplasia,
World Journal of Laparoscopic Surgery, May-August 2011;4(2):123-128 125