
Page 43 - Journal of WALS
P. 43
Ravikumar S
operative working space. The balloon dissector used in this OPERATIVE TECHNIQUE
technique (Fig. 2) has a capacity of 300 cc balloon with a SEPS procedure is performed under general/spinal anesthesia
protective removable cover, a guide rod to aid in introduction with the patient supine and in the trendelenburg position with
and placement and also a 10 mm laparoscopic cannula with skin knee slightly flexed and elevated. In anticipation of concomitant
seal. stripping of superficial veins, the entire extremity is prepared
A second important but optional instrument is the 5 mm circumferentially.
roticulating endograsper (US Surgical, Norwalk, CT, USA) A 10 mm incision is made through the skin, which is 4 cm
(Fig. 3A), where in the tip articulates and rotates which offers a medial to the tibia and 10 to 12 cm below the popliteal crease.
high degree of maneuverability. Subcutaneous tissue is dissected, the posterior compartment
The 5 mm clip applier (Ethicon Endosurgery, Cincinnati,
OH, USA) (Fig. 3B) needs a 5 mm port. Its small size also offers is identified and a 10 mm transverse incision is made into the
a high degree of maneuverability and visibility when working in fascia.
The subfascial space is identified and retractors are placed
a small endoscopic space. The applier delivers 8 mm long
(medium/large) clip in a convenient and with multifire to keep it open.
configuration. The balloon dissector is introduced into the fascial incision
and directed towards the medial malleolus (Figs 4A and 6A).
PREOPERATIVE PREPARATION After removal of balloon cover sheath, the dissection balloon
is inflated with 200 to 300 cc saline. The balloon is designed in
Preoperative evaluation includes color Doppler scanning which
can be used to document superficial, deep, or perforator such a way that initial radial expansion occurs, followed by
incompetence and guide the operative intervention. distal expansion towards the malleolus (Fig. 4B), as the balloon
Incompetent perforator on the skin is accurately mapped and everts distally. Dissection occurs along planes of least
marked which is mandatory as this assists the surgeon during resistance by balloon, hence, the perforating veins are not
surgery. Ultrasonologist can help by marking the sites of disrupted in the dissection process.
incompetent perforators and also that of an incompetent SP The balloon is deflated and removed once the dissection is
junction with the help of a skin marker. accomplished, the rotating seal of 10 mm trocar is secured to
the fascial incision. The cannula is introduced into the space
dissected, and the guide rod and obturator are removed. The
skin seal is rotated into the fascial incision to provide a gas
seal. CO is then insufflated at a pressure of 15 mm Hg to create
2
the working space. A 0º 10 mm rigid laparoscope with attached
video camera and light cable are introduced (Figs 5A and 6B),
and the subfascial space is visualized (Fig. 6C) on the video
monitor.
A working 5 mm laparoscopic port is then inserted in the mid
calf under direct endoscopic guidance. This trocar is placed as
posteriorly as possible to make a wide working axis. This
arrangement of trocar aids visualization of the working instrument
and facilitates instrument manipulation (endograsp dissector or
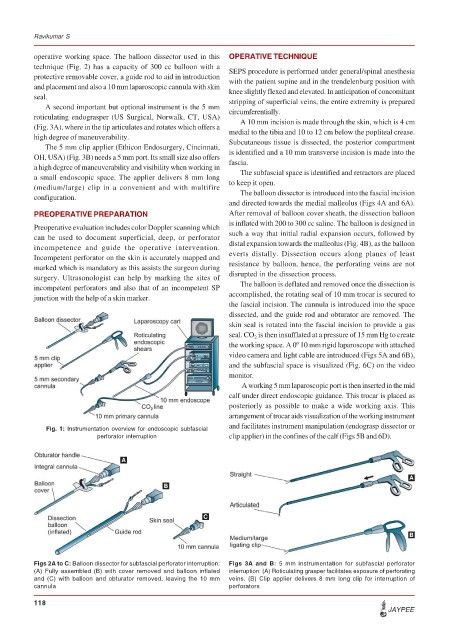
Fig. 1: Instrumentation overview for endoscopic subfascial
perforator interruption clip applier) in the confines of the calf (Figs 5B and 6D).
A
A
B
C
B
Figs 2A to C: Balloon dissector for subfascial perforator interruption: Figs 3A and B: 5 mm instrumentation for subfascial perforator
(A) Fully assembled (B) with cover removed and balloon inflated interruption: (A) Roticulating grasper facilitates exposure of perforating
and (C) with balloon and obturator removed, leaving the 10 mm veins. (B) Clip applier delivers 8 mm long clip for interruption of
cannula perforators
118
JAYPEE