
Page 41 - Journal of Laparoscopic Surgery
P. 41
William Wachira Kibe
difficult ‘open’ cholecystectomy because it minimizes the risks
9
of damage to the structures in or around Calot’s triangle and
has been recommended by many authors for laparoscopic
cholecystectomy for MS types I and II.
The literature reviewed revealed that the papers were all
case reports or case series and therefore a randomized controlled
study comparing the open with the laparoscopic approach is
currently lacking in the surgical literature. 8
ACKNOWLEDGMENT
I would like to acknowledge the assistance and encouragement
I received from Professor RK Mishra who supervised this work.
This review and indeed the whole training would not have been
possible without him and the magnificent team at World
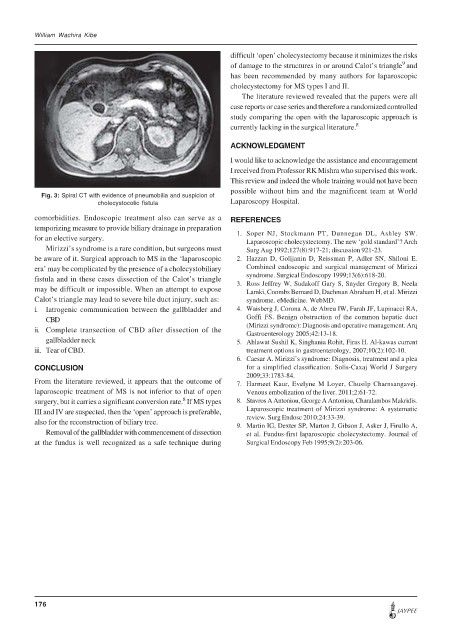
Fig. 3: Spiral CT with evidence of pneumobilia and suspicion of
cholecystocolic fistula Laparoscopy Hospital.
comorbidities. Endoscopic treatment also can serve as a REFERENCES
temporizing measure to provide biliary drainage in preparation
for an elective surgery. 1. Soper NJ, Stockmann PT, Dunnegan DL, Ashley SW.
Laparoscopic cholecystectomy. The new ‘gold standard’? Arch
Mirizzi’s syndrome is a rare condition, but surgeons must Surg Aug 1992;127(8):917-21; discussion 921-23.
be aware of it. Surgical approach to MS in the ‘laparoscopic 2. Hazzan D, Golijanin D, Reissman P, Adler SN, Shiloni E.
era’ may be complicated by the presence of a cholecystobiliary Combined endoscopic and surgical management of Mirizzi
syndrome. Surgical Endoscopy 1999;13(6):618-20.
fistula and in these cases dissection of the Calot’s triangle 3. Ross Jeffrey W, Sudakoff Gary S, Snyder Gregory B, Neela
may be difficult or impossible. When an attempt to expose Lamki, Coombs Bernard D, Dachman Abraham H, et al. Mirizzi
Calot’s triangle may lead to severe bile duct injury, such as: syndrome. eMedicine. WebMD.
i. Iatrogenic communication between the gallbladder and 4. Waisberg J, Corona A, de Abreu IW, Farah JF, Lupinacci RA,
CBD Goffi FS. Benign obstruction of the common hepatic duct
ii. Complete transection of CBD after dissection of the (Mirizzi syndrome): Diagnosis and operative management. Arq
Gastroenterology 2005;42:13-18.
gallbladder neck 5. Ahlawat Sushil K, Singhania Rohit, Firas H. Al-kawas current
iii. Tear of CBD. treatment options in gastroenterology, 2007;10(2):102-10.
6. Caesar A. Mirizzi’s syndrome: Diagnosis, treatment and a plea
CONCLUSION for a simplified classification. Solis-Caxaj World J Surgery
2009;33:1783-84.
From the literature reviewed, it appears that the outcome of 7. Harmeet Kaur, Evelyne M Loyer, Chusilp Charnsangavej.
laparoscopic treatment of MS is not inferior to that of open Venous embolization of the liver. 2011;2:61-72.
8
surgery, but it carries a significant conversion rate. If MS types 8. Stavros A Antoniou, George A Antoniou, Charalambos Makridis.
III and IV are suspected, then the ‘open’ approach is preferable, Laparoscopic treatment of Mirizzi syndrome: A systematic
review. Surg Endosc 2010;24:33-39.
also for the reconstruction of biliary tree. 9. Martin IG, Dexter SP, Marton J, Gibson J, Asker J, Firullo A,
Removal of the gallbladder with commencement of dissection et al. Fundus-first laparoscopic cholecystectomy. Journal of
at the fundus is well recognized as a safe technique during Surgical Endoscopy Feb 1995;9(2):203-06.
176
JAYPEE