
Page 4 - Journal of Laparoscopic Surgery
P. 4
Ali Aminian et al
of newly developed instruments and techniques may expose dissection of gallbladder from its bed is started by the help of
patients to additional risk. 1,3 hook. It may be necessary to change the place of second traction
suture from right side of abdomen to epigastric area in order to
OPERATIVE TECHNIQUE get better visualization of gallbladder bed (Figs 4A to D). At the
After initial experience in pig model, this procedure was end of dissection, irrigation and suction and control of
performed in human. Patients with normal body mass index and hemostasis are performed (Fig. 5A). Grasping forceps is
with no previous history of acute cholecystitis are suitable introduced through supraumbilical port and the gallbladder is
candidates for elective scarless LC. Preoperative preparations removed under direct vision (Figs 5B to D). The periumbilical
are similar to standard LC. fascia and skin are closed. Postoperative care is similar to
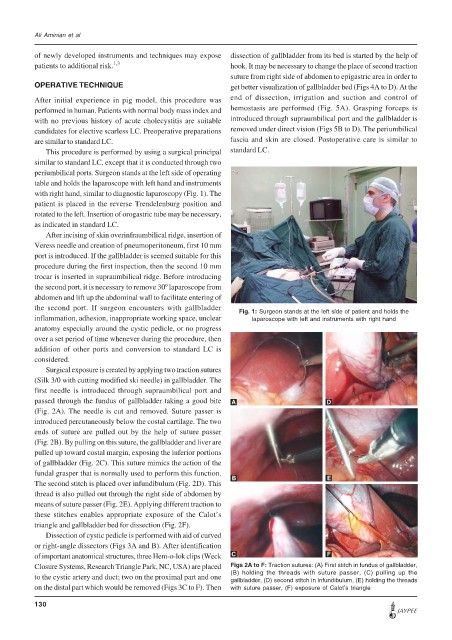
This procedure is performed by using a surgical principal standard LC.
similar to standard LC, except that it is conducted through two
periumbilical ports. Surgeon stands at the left side of operating
table and holds the laparoscope with left hand and instruments
with right hand, similar to diagnostic laparoscopy (Fig. 1). The
patient is placed in the reverse Trendelenburg position and
rotated to the left. Insertion of orogastric tube may be necessary,
as indicated in standard LC.
After incising of skin overinfraumbilical ridge, insertion of
Veress needle and creation of pneumoperitoneum, first 10 mm
port is introduced. If the gallbladder is seemed suitable for this
procedure during the first inspection, then the second 10 mm
trocar is inserted in supraumbilical ridge. Before introducing
the second port, it is necessary to remove 30º laparoscope from
abdomen and lift up the abdominal wall to facilitate entering of
the second port. If surgeon encounters with gallbladder
Fig. 1: Surgeon stands at the left side of patient and holds the
inflammation, adhesion, inappropriate working space, unclear laparoscope with left and instruments with right hand
anatomy especially around the cystic pedicle, or no progress
over a set period of time whenever during the procedure, then
addition of other ports and conversion to standard LC is
considered.
Surgical exposure is created by applying two traction sutures
(Silk 3/0 with cutting modified ski needle) in gallbladder. The
first needle is introduced through supraumbilical port and
passed through the fundus of gallbladder taking a good bite A D
(Fig. 2A). The needle is cut and removed. Suture passer is
introduced percutaneously below the costal cartilage. The two
ends of suture are pulled out by the help of suture passer
(Fig. 2B). By pulling on this suture, the gallbladder and liver are
pulled up toward costal margin, exposing the inferior portions
of gallbladder (Fig. 2C). This suture mimics the action of the
fundal grasper that is normally used to perform this function.
The second stitch is placed over infundibulum (Fig. 2D). This B E
thread is also pulled out through the right side of abdomen by
means of suture passer (Fig. 2E). Applying different traction to
these stitches enables appropriate exposure of the Calot’s
triangle and gallbladder bed for dissection (Fig. 2F).
Dissection of cystic pedicle is performed with aid of curved
or right-angle dissectors (Figs 3A and B). After identification
of important anatomical structures, three Hem-o-lok clips (Weck C F
Closure Systems, Research Triangle Park, NC, USA) are placed Figs 2A to F: Traction sutures: (A) First stitch in fundus of gallbladder,
to the cystic artery and duct; two on the proximal part and one (B) holding the threads with suture passer, (C) pulling up the
gallbladder, (D) second stitch in infundibulum, (E) holding the threads
on the distal part which would be removed (Figs 3C to F). Then with suture passer, (F) exposure of Calot’s triangle
130
JAYPEE