
Page 9 - Laparoscopic Surgery Online Journal
P. 9
WJOLS
Laparoscopic Management of Perforated Peptic Ulcer in Early and Late Presentation: A Comparative Study
15 were female. In our study we took early presentation as
3 days and late presentation as 3 to 7 days (time taken for
seeking treatment from the onset of symptoms). Thirty-seven
presented early whereas other 21 presented late. All patients
were compared for variables like operating time,
intraoperative complications, risk of anesthesia, rate of
conversion to open surgery, postoperative pain and the opiate
analgesic requirements, postoperative morbidity and
mortality, hospital stay. Postoperative follow-up was done
at 1, 6 months, 1 year and yearly thereafter.
After initial resuscitation and investigation revealing gas
under diaphragm in straight X-ray of abdomen, patients were
posted for surgery.
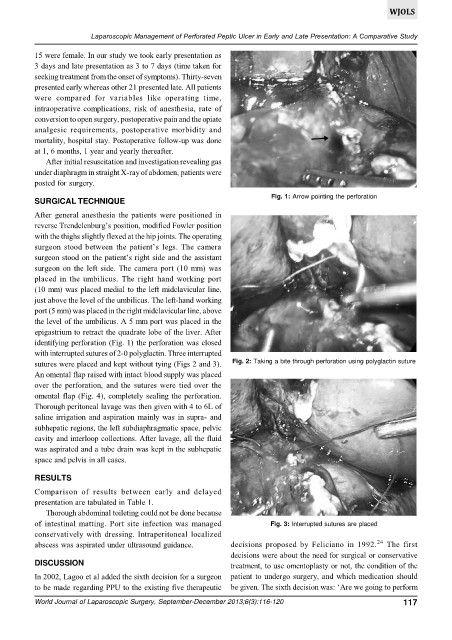
Fig. 1: Arrow pointing the perforation
SURGICAL TECHNIQUE
After general anesthesia the patients were positioned in
reverse Trendelenburg’s position, modified Fowler position
with the thighs slightly flexed at the hip joints. The operating
surgeon stood between the patient’s legs. The camera
surgeon stood on the patient’s right side and the assistant
surgeon on the left side. The camera port (10 mm) was
placed in the umbilicus. The right hand working port
(10 mm) was placed medial to the left midclavicular line,
just above the level of the umbilicus. The left-hand working
port (5 mm) was placed in the right midclavicular line, above
the level of the umbilicus. A 5 mm port was placed in the
epigastrium to retract the quadrate lobe of the liver. After
identifying perforation (Fig. 1) the perforation was closed
with interrupted sutures of 2-0 polyglactin. Three interrupted
sutures were placed and kept without tying (Figs 2 and 3). Fig. 2: Taking a bite through perforation using polyglactin suture
An omental flap raised with intact blood supply was placed
over the perforation, and the sutures were tied over the
omental flap (Fig. 4), completely sealing the perforation.
Thorough peritoneal lavage was then given with 4 to 6L of
saline irrigation and aspiration mainly was in supra- and
subhepatic regions, the left subdiaphragmatic space, pelvic
cavity and interloop collections. After lavage, all the fluid
was aspirated and a tube drain was kept in the subhepatic
space and pelvis in all cases.
RESULTS
Comparison of results between early and delayed
presentation are tabulated in Table 1.
Thorough abdominal toileting could not be done because
of intestinal matting. Port site infection was managed Fig. 3: Interrupted sutures are placed
conservatively with dressing. Intraperitoneal localized
24
abscess was aspirated under ultrasound guidance. decisions proposed by Feliciano in 1992. The first
decisions were about the need for surgical or conservative
DISCUSSION treatment, to use omentoplasty or not, the condition of the
In 2002, Lagoo et al added the sixth decision for a surgeon patient to undergo surgery, and which medication should
to be made regarding PPU to the existing five therapeutic be given. The sixth decision was: ‘Are we going to perform
World Journal of Laparoscopic Surgery, September-December 2013;6(3):116-120 117