
Page 5 - Laparoscopic Surgery Online Journal
P. 5
WJOLS
Laparoscopy: A Procedure no less than Laparotomy for Lymph Node Dissection in Total Gastrectomy for Gastric Carcinoma
worldwide. 19 In Eastern Asian countries such as Japan,
China, and Korea, D2 dissection has been the standard
20
operation. However, in Western countries, D2 dissection
is thought to be accompanied by significant mortality and
morbidity, with no survival advantage. 21-23 Hartgrink et al 22
reported the results of a Dutch gastric cancer group trial in
2004, which included 711 patients who underwent randomly
assigned treatment with curative intent (380 in D1 and 331
in D2). Both the postoperative morbidity (25 vs 43%,
p < 0.001) and mortality (4 vs 10%, p = 0.004) were
significantly higher in patients who underwent D2
dissection, while there was no difference in the 11-year
overall survival (30 vs 35%, p = 0.53) between the two
groups. Those results were similar to that of the Medical
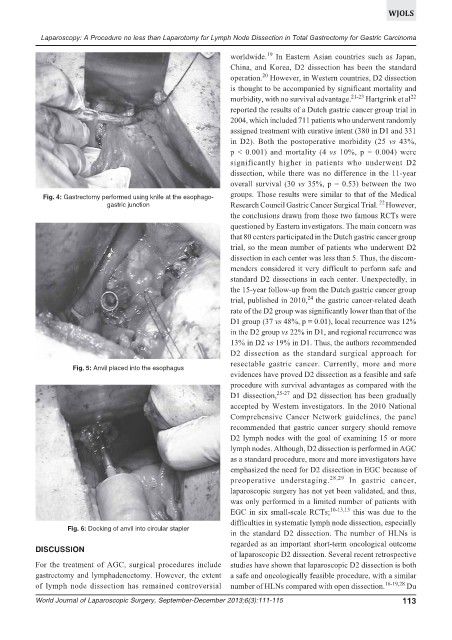
Fig. 4: Gastrectomy performed using knife at the esophago-
22
gastric junction Research Council Gastric Cancer Surgical Trial. However,
the conclusions drawn from those two famous RCTs were
questioned by Eastern investigators. The main concern was
that 80 centers participated in the Dutch gastric cancer group
trial, so the mean number of patients who underwent D2
dissection in each center was less than 5. Thus, the discom-
menders considered it very difficult to perform safe and
standard D2 dissections in each center. Unexpectedly, in
the 15-year follow-up from the Dutch gastric cancer group
24
trial, published in 2010, the gastric cancer-related death
rate of the D2 group was significantly lower than that of the
D1 group (37 vs 48%, p = 0.01), local recurrence was 12%
in the D2 group vs 22% in D1, and regional recurrence was
13% in D2 vs 19% in D1. Thus, the authors recommended
D2 dissection as the standard surgical approach for
resectable gastric cancer. Currently, more and more
Fig. 5: Anvil placed into the esophagus
evidences have proved D2 dissection as a feasible and safe
procedure with survival advantages as compared with the
D1 dissection, 25-27 and D2 dissection has been gradually
accepted by Western investigators. In the 2010 National
Comprehensive Cancer Network guidelines, the panel
recommended that gastric cancer surgery should remove
D2 lymph nodes with the goal of examining 15 or more
lymph nodes. Although, D2 dissection is performed in AGC
as a standard procedure, more and more investigators have
emphasized the need for D2 dissection in EGC because of
preoperative understaging. 28,29 In gastric cancer,
laparoscopic surgery has not yet been validated, and thus,
was only performed in a limited number of patients with
EGC in six small-scale RCTs; 10-13,15 this was due to the
difficulties in systematic lymph node dissection, especially
Fig. 6: Docking of anvil into circular stapler
in the standard D2 dissection. The number of HLNs is
regarded as an important short-term oncological outcome
DISCUSSION
of laparoscopic D2 dissection. Several recent retrospective
For the treatment of AGC, surgical procedures include studies have shown that laparoscopic D2 dissection is both
gastrectomy and lymphadenectomy. However, the extent a safe and oncologically feasible procedure, with a similar
of lymph node dissection has remained controversial number of HLNs compared with open dissection. 16-19,28 Du
World Journal of Laparoscopic Surgery, September-December 2013;6(3):111-115 113