
Page 48 - WJOLS
P. 48
Medhat M Ibrahim et al
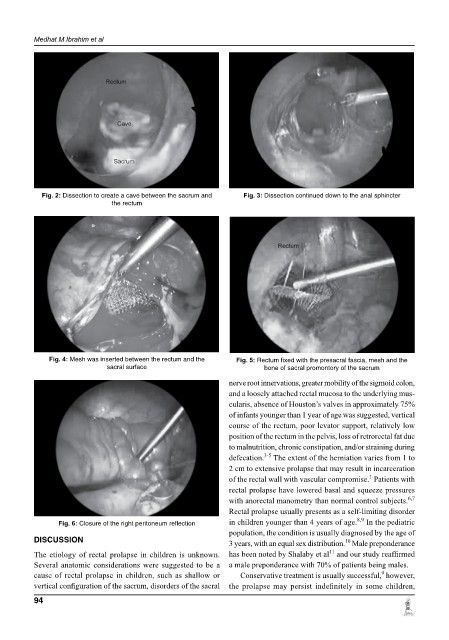
Fig. 2: Dissection to create a cave between the sacrum and Fig. 3: Dissection continued down to the anal sphincter
the rectum
Fig. 4: Mesh was inserted between the rectum and the Fig. 5: Rectum fixed with the presacral fascia, mesh and the
sacral surface bone of sacral promontory of the sacrum
nerve root innervations, greater mobility of the sigmoid colon,
and a loosely attached rectal mucosa to the underlying mus-
cularis, absence of Houston’s valves in approximately 75%
of infants younger than 1 year of age was suggested, vertical
course of the rectum, poor levator support, relatively low
position of the rectum in the pelvis, loss of retrorectal fat due
to malnutrition, chronic constipation, and/or straining during
3-5
defecation. The extent of the herniation varies from 1 to
2 cm to extensive prolapse that may result in incarceration
1
of the rectal wall with vascular compromise. Patients with
rectal prolapse have lowered basal and squeeze pressures
6,7
with anorectal manometry than normal control subjects.
Rectal prolapse usually presents as a self-limiting disorder
8,9
Fig. 6: Closure of the right peritoneum reflection in children younger than 4 years of age. In the pediatric
population, the condition is usually diagnosed by the age of
diSCUSSion 3 years, with an equal sex distribution. Male preponderance
10
11
The etiology of rectal prolapse in children is unknown. has been noted by Shalaby et al and our study reaffirmed
Several anatomic considerations were suggested to be a a male preponderance with 70% of patients being males.
9
cause of rectal prolapse in children, such as shallow or Conservative treatment is usually successful, however,
vertical configuration of the sacrum, disorders of the sacral the prolapse may persist indefinitely in some children,
94