
Page 31 - WJOLS
P. 31
WJOLS
Is there an Ideal Port Position for Laparoscopic Urological Procedures?
29
37
ports, most especially when it is to be robotic assisted port while others described umbilical primary port and
others described the distance of the second and third ports both lower abdominal quadrants ports. 38,39
to be 8 to 10 cm from the camera port. 30
Transumbilical LESS radical prostatectomy was first Mitrofanoff
described in 2008 by Kaouk et al, through the umbilicus A fourport transperitoneal approach is described, with
using a single threechannel port, and 2 years later Desai camera at umbilicus, two 5 mm at left lower quadrant and
et al published the initial series of singleport transvesical right midaxillary line at the level of the umbilicus. Fourth
simple prostatectomy where a singleport device inserted port at left midaxillary also at umbilical level. 40
percutaneously into the bladder through a 2 to 3 cm incision
in the suprapubic skin crease was used. 5 other LESS Procedures
Laparoscopic Cystectomy Single site laparoscopic surgery has been reported in small
numbers for a variety of other urological conditions. A mesh
Laparoscopic cystectomy has been described by many sling has been successfully removed from the bladder via a
authors, but remains to be evaluated and is far from transvesical approach. Sacrocolpopexies, orchidopexy and
being a standard procedure. While some described a similar orchidectomy have been successfully performed through a
approach to prostatectomy with periumbilical port, two single incision without complication. 5
others 8 to 10 cm away from the primary port and then
31
bilateral iliac fossae others described only four ports dISCUSSIon
approach with 3 to 4 cm supraumbilical camera port and
32
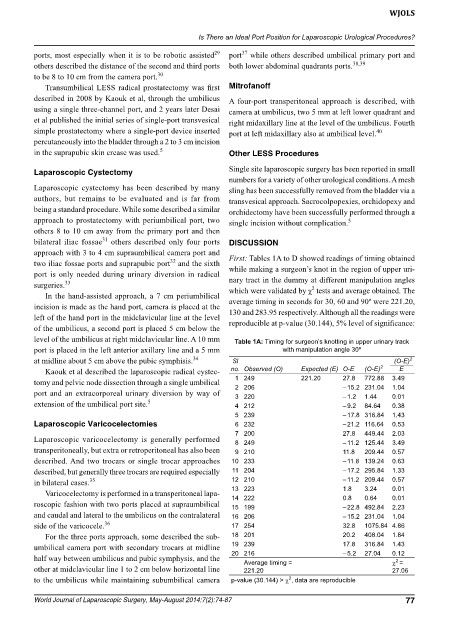
two iliac fossae ports and suprapubic port and the sixth First: Tables 1A to D showed readings of timing obtained
while making a surgeon’s knot in the region of upper uri
port is only needed during urinary diversion in radical nary tract in the dummy at different manipulation angles
surgeries. 33 2
In the handassisted approach, a 7 cm periumbilical which were validated by χ tests and average obtained. The
average timing in seconds for 30, 60 and 90º were 221.20,
incision is made as the hand port, camera is placed at the 130 and 283.95 respectively. Although all the readings were
left of the hand port in the midclavicular line at the level
of the umbilicus, a second port is placed 5 cm below the reproducible at pvalue (30.144), 5% level of significance:
level of the umbilicus at right midclavicular line. A 10 mm Table 1A: Timing for surgeon’s knotting in upper urinary track
port is placed in the left anterior axillary line and a 5 mm with manipulation angle 30º
at midline about 5 cm above the pubic symphisis. 34 Sl (O-E) 2
Kaouk et al described the laparoscopic radical cystec no. Observed (O) Expected (E) O-E (O-E) 2 E
tomy and pelvic node dissection through a single umbilical 1 249 221.20 27.8 772.88 3.49
2 206
1.04
– 15.2 231.04
port and an extracorporeal urinary diversion by way of 3 220 – 1.2 1.44 0.01
extension of the umbilical port site. 5 4 212 – 9.2 84.64 0.38
5 239 – 17.8 316.84 1.43
Laparoscopic Varicocelectomies 6 232 – 21.2 116.64 0.53
7 200 27.8 449.44 2.03
Laparoscopic varicocelectomy is generally performed 8 249 – 11.2 125.44 3.49
transperitoneally, but extra or retroperitoneal has also been 9 210 11.8 209.44 0.57
described. And two trocars or single trocar approaches 10 233 – 11.8 139.24 0.63
described, but generally three trocars are required especially 11 204 – 17.2 295.84 1.33
in bilateral cases. 35 12 210 – 11.2 209.44 0.57
Varicocelectomy is performed in a transperitoneal lapa 13 223 1.8 3.24 0.01
14 222
0.01
0.8
0.64
roscopic fashion with two ports placed at supraumbilical 15 199 – 22.8 492.84 2.23
and caudal and lateral to the umbilicus on the contralateral 16 206 – 15.2 231.04 1.04
side of the varicocele. 36 17 254 32.8 1075.84 4.86
For the three ports approach, some described the sub 18 201 20.2 408.04 1.84
umbilical camera port with secondary trocars at midline 19 239 17.8 316.84 1.43
half way between umbilicus and pubic symphysis, and the 20 216 – 5.2 27.04 0.12
2
c =
Average timing =
other at midclavicular line 1 to 2 cm below horizontal line 221.20 27.06
2
to the umbilicus while maintaining subumbilical camera p-value (30.144) > c , data are reproducible
World Journal of Laparoscopic Surgery, May-August 2014;7(2):74-87 77