
Page 4 - World Journal of Laparoscopic Surgery
P. 4
Aswini Kumar Misro, Prakash Sapkota
between falciform ligament and the anterior peritoneum. freedom of the port 3 around port 2 helps in traction
A 5 mm grasper (with reducer) is introduced through and dissection to be done at various points and depth
the port 2 and the fundus of the gallbladder is grasped (However the rotation of the port should never be
and traction is applied toward the right shoulder. This attempted with the instrument inside the port) (Figs 2
step displays the gallbladder anatomy in entirety. Now and 3). The cystic artery and duct is circumferentially
an intraoperative assessment is done to determine if skeletonized. With double clips placed on the body side
the 2 port laparoscopic cholecystectomy can be done safely and a single clip on the specimen side, both the structures
(patient suitability has been described in discu ssion). are divided. This step is completed by traction through
If conditions are found to be favorable, with the trac- the port 3 instrument and clip application through port 2.
tion maintained in the described way, a 5 mm port is With continued traction applied to the Hartman’s pouch
inserted through the existing epigastric skin incision in the upward and right direction (this open up the
(but through a separate stab traversing a different path interface between the gallbladder and the gallbladder
to the peritoneal cavity) little away from the port 2 fossa of the liver), the gallbladder is separated from the
pointing toward the Hartman’s pouch of the gallbladder gallbladder fossa by electrodissection with an appropriate
(This will be referred henceforth as port 3) (Figs 1 and 2). instrument (either a monopolar hook, Maryland or scissor).
Prior to this step, the skin incision may be extended 3 to Before the final detachment of gallbladder from liver, the
5 mm or more as required. hemostasis of the gallbladder bed is achieved and the
Now appropriate traction is applied to the Hartman’s cystic pedicle (artery and duct) security is confirmed.
pouch in lateral direction by the port 3 instrument, and The 5 mm port is now withdrawn and the specimen
this widens up the Calot’s triangle. With a suitable instru- extracted through the epigastric port. Generous amount
ment (preferably a Maryland introduced through the of peritoneal wash is given and 100 ml of normal saline
port 2), Calot’s triangle dissection is done. The traction and mixed with bupivacaine is left in the subdiaphragmatic
dissection instruments are used interchangeably through space. Pneumoperitonium is evacuated and the wounds
the port 2 and 3 as per requirement. The rotational closed in 2 layers.
Due to the presence of two ports in the same wound
the range of their movement is likely to be affected.
Hence, careful attention should be paid to proper align-
ment of the ports at the epigastric site. The chamber of
the 5 mm port should be as close to the skin as possible
where as that of 10 mm port should be as far away from
the skin as possible (Figs 1 to 3). The maneuverability and
the freedom of a port depend on the rotational capacity
or the swing of the ports. With the measures mentioned
above, we have observed that there is adequate overall
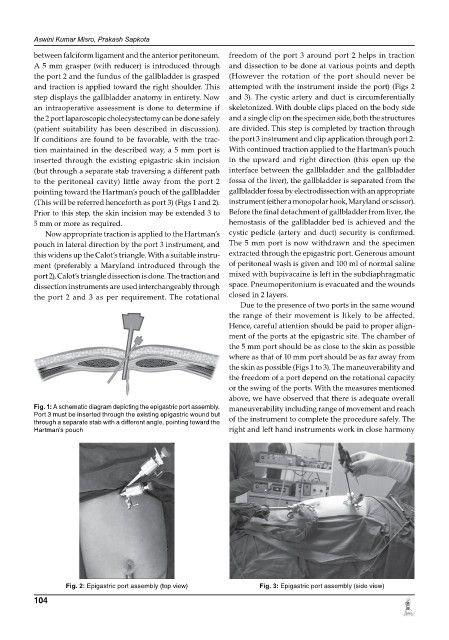
Fig. 1: A schematic diagram depicting the epigastric port assembly. maneuverability including range of movement and reach
Port 3 must be inserted through the existing epigastric wound but of the instrument to complete the procedure safely. The
through a separate stab with a different angle, pointing toward the
Hartman’s pouch right and left hand instruments work in close harmony
Fig. 2: Epigastric port assembly (top view) Fig. 3: Epigastric port assembly (side view)
104