
Page 12 - World Journal of Laparoscopic Surgery
P. 12
A Rubbia et al
surgical intervention. Also in a developing country like and pelvic tuberculosis were the main pathologic find-
20
ours where advanced radiological investigations are ings followed by appendicitis. This was also reported
15
beyond the scope of grass root level medical practice by A Gupta et al who gave a diagnostic accuracy of 92%
(often not readily available and costly) this approach only where abdominal tuberculosis and gynecological patho-
serves to increase cost and delay treatment. Diagnostic logy were the most common diagnoses. This only serves
laparoscopy should, thus, be considered as step II of the to confirm the increased prevalence of tuberculosis in
14
21
management. the subcontinent. Easter et al, however, reported a high
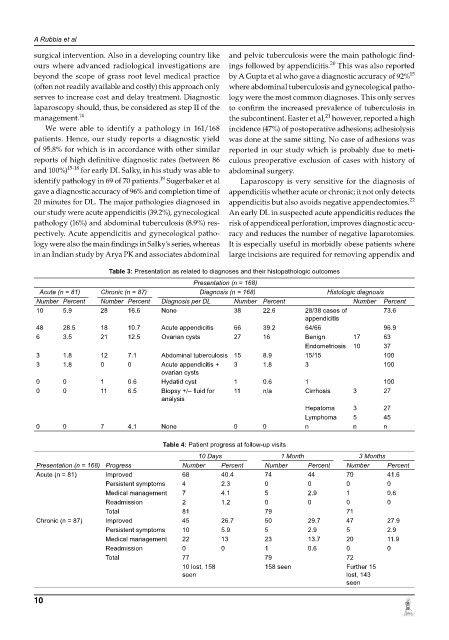
We were able to identify a pathology in 161/168 incidence (47%) of postoperative adhesions; adhesiolysis
patients. Hence, our study reports a diagnostic yield was done at the same sitting. No case of adhesions was
of 95.8% for which is in accordance with other similar reported in our study which is probably due to meti-
reports of high definitive diagnostic rates (between 86 culous preoperative exclusion of cases with history of
and 100%) 1518 for early DL Salky, in his study was able to abdominal surgery.
19
identify pathology in 69 of 70 patients. Sugerbaker et al Laparoscopy is very sensitive for the diagnosis of
gave a diagnostic accuracy of 96% and completion time of appendicitis whether acute or chronic; it not only detects
22
20 minutes for DL. The major pathologies diagnosed in appendicitis but also avoids negative appendectomies.
our study were acute appendicitis (39.2%), gynecological An early DL in suspected acute appendicitis reduces the
pathology (16%) and abdominal tuberculosis (8.9%) res- risk of appendiceal perforation, improves diagnostic accu-
pectively. Acute appendicitis and gynecological patho- racy and reduces the number of negative laparotomies.
logy were also the main findings in Salky’s series, whereas It is especially useful in morbidly obese patients where
in an Indian study by Arya PK and associates abdominal large incisions are required for removing appendix and
Table 3: Presentation as related to diagnoses and their histopathologic outcomes
Presentation (n = 168)
Acute (n = 81) Chronic (n = 87) Diagnosis (n = 168) Histologic diagnosis
Number Percent Number Percent Diagnosis per DL Number Percent Number Percent
10 5.9 28 16.6 None 38 22.6 28/38 cases of 73.6
appendicitis
48 28.5 18 10.7 Acute appendicitis 66 39.2 64/66 96.9
6 3.5 21 12.5 Ovarian cysts 27 16 Benign 17 63
Endometriosis 10 37
3 1.8 12 7.1 Abdominal tuberculosis 15 8.9 15/15 100
3 1.8 0 0 Acute appendicitis + 3 1.8 3 100
ovarian cysts
0 0 1 0.6 Hydatid cyst 1 0.6 1 100
0 0 11 6.5 Biopsy +/– fluid for 11 n/a Cirrhosis 3 27
analysis
Hepatoma 3 27
Lymphoma 5 45
0 0 7 4.1 None 0 0 n n n
Table 4: Patient progress at followup visits
10 Days 1 Month 3 Months
Presentation (n = 168) Progress Number Percent Number Percent Number Percent
Acute (n = 81) Improved 68 40.4 74 44 70 41.6
Persistent symptoms 4 2.3 0 0 0 0
Medical management 7 4.1 5 2.9 1 0.6
Readmission 2 1.2 0 0 0 0
Total 81 79 71
Chronic (n = 87) Improved 45 26.7 50 29.7 47 27.9
Persistent symptoms 10 5.9 5 2.9 5 2.9
Medical management 22 13 23 13.7 20 11.9
Readmission 0 0 1 0.6 0 0
Total 77 79 72
10 lost, 158 158 seen Further 15
seen lost, 143
seen
10