
Page 9 - Journal of Laparoscopic Surgery - WALS Journal
P. 9
WJOLS
Can Intraperitoneal Tramadol decrease Pain in Patients undergoing Laparoscopic Cholecystectomy
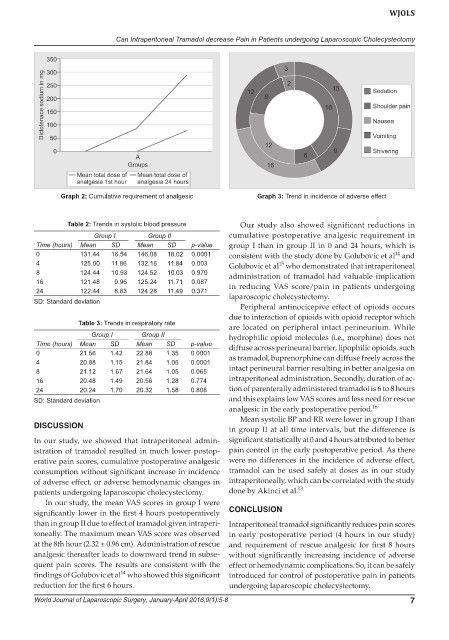
Graph 2: Cumulative requirement of analgesic Graph 3: Trend in incidence of adverse effect
Table 2: Trends in systolic blood pressure Our study also showed significant reductions in
Group I Group II cumulative postoperative analgesic requirement in
Time (hours) Mean SD Mean SD p-value group I than in group II in 0 and 24 hours, which is
0 131.44 16.54 146.08 18.02 0.0001 consistent with the study done by Golubovic et al and
14
4 125.00 11.86 132.16 11.84 0.003 Golubovic et al who demonstrated that intraperitoneal
15
8 124.44 10.93 124.52 10.03 0.970 administration of tramadol had valuable implication
16 121.48 9.96 125.24 11.71 0.087 in reducing VAS score/pain in patients undergoing
24 122.44 8.83 124.28 11.49 0.371
SD: Standard deviation laparoscopic cholecystectomy.
Peripheral antinocicepive effect of opioids occurs
due to interaction of opioids with opioid receptor which
Table 3: Trends in respiratory rate
are located on peripheral intact perineurium. While
Group I Group II hydrophilic opioid molecules (i.e., morphine) does not
Time (hours) Mean SD Mean SD p-value diffuse across perineural barrier, lipophilic opioids, such
0 21.56 1.42 22.88 1.35 0.0001 as tramadol, buprenorphine can diffuse freely across the
4 20.88 1.15 21.84 1.06 0.0001
8 21.12 1.67 21.64 1.05 0.065 intact perineural barrier resulting in better analgesia on
16 20.48 1.49 20.56 1.28 0.774 intraperitoneal administration. Secondly, duration of ac-
24 20.24 1.70 20.32 1.58 0.808 tion of parenterally administered tramadol is 6 to 8 hours
SD: Standard deviation and this explains low VAS scores and less need for rescue
analgesic in the early postoperative period. 16
Mean systolic BP and RR were lower in group I than
DISCUSSION
in group II at all time intervals, but the difference is
In our study, we showed that intraperitoneal admin- significant statistically at 0 and 4 hours attributed to better
istration of tramadol resulted in much lower postop- pain control in the early postoperative period. As there
erative pain scores, cumulative postoperative analgesic were no differences in the incidence of adverse effect,
consumption without significant increase in incidence tramadol can be used safely at doses as in our study
of adverse effect, or adverse hemodynamic changes in intraperitoneally, which can be correlated with the study
patients undergoing laparoscopic cholecystectomy. done by Akinci et al. 13
In our study, the mean VAS scores in group I were
significantly lower in the first 4 hours postoperatively CONCLUSION
than in group II due to effect of tramadol given intraperi- Intraperitoneal tramadol significantly reduces pain scores
toneally. The maximum mean VAS score was observed in early postoperative period (4 hours in our study)
at the 8th hour (2.32 ± 0.96 cm). Administration of rescue and requirement of rescue analgesic for first 8 hours
analgesic thereafter leads to downward trend in subse- without significantly increasing incidence of adverse
quent pain scores. The results are consistent with the effect or hemodynamic complications. So, it can be safely
14
findings of Golubovic et al who showed this significant introduced for control of postoperative pain in patients
reduction for the first 6 hours. undergoing laparoscopic cholecystectomy.
World Journal of Laparoscopic Surgery, January-April 2016;9(1):5-8 7