DR AKRAM ALLOUBANI
G. SURGEON, JORDANIAN BOARD Member of world association of laparoscopic surgeonsDiploma in Minimal Access surgery
Project Submitted Towards Completion Of Diploma In Minimal Access Surgery, World Laparoscopy Hospital, Gurugram, NCR Delhi, India. Sep 2007.
Click Here to Use Our BMI Calculator
Abstract: Obesity is a major health care problem, In U. S .A. 30 million overweight, 7 million morbidly obese. Cost for management of Bariatric comorbidities in states $ 100 billion annuallyWeight reduction surgery is performed by either the open or laparoscopic approach, improves health outcomes of morbidly obese patients by leading to substantial weight loss with relatively low rates of adverse events. In my study, Iam discussing different approach of laparoscopic Weight reduction operations, comparing between technique, advantage, disadvantage, complication and long term benefit.
Key words: Obesity, Laparoscopic approachs,bariatric , comparison
Introduction: Morbid obesity is defined as a body mass index (BMI) greater than 40 kg/m2. The prevalence of morbid obesity in the U.S. is 6% for women and 2% for men; morbid obesity is associated with a shortened life span. For example, a morbidly obese man at age 20 can expect to live 13 years less than his counterpart with a normal BMI, which equates to a 22% reduction in life expectancy.
Classification of obesity
Obesity class BMI (kg/m2)
Underweight! 18.5Normal 18.5–24.9Overweight 25.0–29.9Mild obesity I 30.0–34.9Moderate obesity II 35.0–39.9Severe obesity III R40.0
Materials and methods: A literature search was performed using search engine Google, HighWire Press, SpringerLink and library facility available at laparoscopic hospital. The following search terms was used: laparoscopic _ bariatric. Criteria for selection of papers were upon statistical way of analysis, institute if they were specialized for laparoscopy, the way of management and the technique of operations
Pathophysiology- Not Clear - Genetic Factor- Metabolism - Endocrine regulation - Psychosocial & culturalThe basic mechanism is (( Energy Intake > Energy output ))
Complications of obesityRisk Factor for:1- Coronary artery disease2- Type II Diabetes Mellitus.3- Hypertension. 4- Dyslipidemia.5- Gallbladder disease6- GERD.7- Arthritis of W t bearing joints8- Obstructive Sleep apnea9- Psychosocial & Socioeconomic10- Certain Malignancies
Treatment
- Non -surgical: The first treatment of morbid obesity involves dietary and lifestyle changes. Although this strategy may be effective in some patients, frequently the weight loss is not durable, with only 5%-10% of patients able to comply with lifestyle modifications on a long-term basis.
- Conventional ( Non pharmacological): Diet Physical exercise Behavioral therapy
- Pharmacological treatment
- 2 Surgical Treatment: is the only effective long-term treatment for patients with morbid obesity .When conservative measures fail; some patients may consider surgical approaches. A 1991 National Institutes of Health (NIH) Consensus Conference defined surgical candidates as those BMI of greater than 40 kg/m2, or greater than 35 kg/m2 in conjunction with severe co morbidities such as cardiopulmonary complications or severe diabetes. (2) Super obesity has been described as a BMI greater than 50 kg/m2
Indication for Surgery in M. O 1. BMI of 40 & more2. BMI of 35 – 40 with obesity related co morbidities e.g. D.M., HTN, Severe arthritis, Sleep apnea Syndrome. 3. No history of alcohol or drug abuse.4. Age over 18 & under 55 years
Contraindications–Significant psychiatric disorders- Endocrine problem- Inflammatory bowel disease- Severe Organic disease.
Criteria for surgical therapy: 1. Safe, as little invasive as possible.2. Highly efficient i.e. 50% of excess W t. eliminated within 5 Years.3. The operative risk should be lower than the risk of natural evolution of the disease4. Carry few long term ComplicationsEvaluation of patient prior to surgery:Multidisciplinary Team:- Nutritionist- Anesthesiologist- Endocrinologist- Psychiatrist.- SurgeonRationale For Laparoscopic Surgery for M.O.1. Reduce Wound – related complications.2. Shorten hospital stay.3. Decrease postoperative pain4. Improve respiratory function.5. Faster convalescence
Types of Operations for M. O.I. Gastric restrictive procedures *Lap. Vertical banded gastroplasty. *Lap. Adjustable gastric BandingII.Malabsorptive Procedure *Biliopancreatic diversion + duodenal switch , jejuno-ileal Bypass|||.mixed procedure *R – Y Gastrojejunostomy
1) Laparoscopic Vertical Banded Gastroplasty (VBG)- Described in 1994 by Hess .- Purely restrictive procedure with no Malabsorptive component .- Relatively simple operation with low operative risk. -Techniques: In this procedure the stomach is segmented along its vertical axis. To create a durable reinforced and rate-limiting stoma at the distal end of the pouch, a plug of stomach is removed and a propylene collar is placed through this hole and then stapled to itself. Because the normal flow of food is preserved,metabolic complications are rare


Adjustable Gastric Banding - It is the least invasive surgical treatment of Morbid obesity.- Described in 1993 by Catona .- It is purely restrictive procedure .- In Europe ,it is the bariatric procedure of choice.- In U.S.A. ,FDA approval since June 2001 .
-Techniques Adjustable gastric banding involves placing a gastric band around the exterior of the stomach. The band is attached to a reservoir that is implanted subcutaneously in the rectus sheath. Injecting the reservoir with saline alters the diameter of the gastric band; therefore, the rate limiting stoma in the stomach can be progressively narrowed to induce greater weight loss, or expanded if complications develop. Because the stomach is not entered, the surgery and any revisions, if necessary, are relatively simple




Malabsorptive Procedures: There are multiple variants of malabsorptive procedures, which differ in the lengths of the alimentary limb, the biliopancreatic limb, and the common limb, where the alimentary and biliopancreatic limb are anastomosed. These procedures also may include an element of a restrictive surgery based on the size of the stomach pouch. The degree of malabsorption is related to the length of the alimentary and common limbs.
- Biliopancreatic Bypass Procedure (also known as the Scopinaro procedure)
The biliopancreatic bypass (BPB) procedure, developed and used extensively in Italy, was designed to address some of the drawbacks of the original intestinal bypass procedures that have been abandoned due to unacceptable metabolic complications. Many of the complications were thought to be related to bacterial overgrowth and toxin production in the blind, bypassed segment. In contrast, BPB consists of a subtotal gastrectomy and diversion of the biliopancreatic juices into the distal ileum by a long Roux-en-Y procedure. The procedure consists of the following components:
- A distal gastrectomy functions to induce a temporary early satiety and/or the dumping syndrome in the early postoperative period, both of which limit food intake.
- A 200-cm long "alimentary tract" consists of 200 cm of ileum connecting the stomach to a common distal segment.
- A 300- to 400-cm "biliary tract," which connects the duodenum, jejunum, and remaining ileum to the common distal segment.
- A 50- to 100-cm "common tract," where food from the alimentary tract mixes with biliopancreatic juices from the biliary tract. Food digestion and absorption, particularly of fats and starches, are therefore limited to this small segment of bowel, creating a selective malabsorption. The length of the common segment influences the degree of malabsorption.
- Because of the high incidence of cholelithiasis associated with the procedure, patients typically undergo an associated cholecystectomy.
- Biliopancreatic Bypass with Duodenal Switch -
The duodenal switch procedure is essentially a variant of the biliopancreatic bypass described above. However, instead of performing a distal gastrectomy, a "sleeve" gastrectomy is performed along the vertical axis of the stomach, preserving the pylorus and initial segment of the duodenum, which is then anastomosed to a segment of the ileum, similar to the above procedure, to create the alimentary limb. Preservation of the pyloric sphincter is intended to ameliorate the dumping syndrome and decrease the incidence of ulcers at the duodenoileal anastomosis by providing a more physiologic transfer of stomach contents to the duodenum. The sleeve gastrectomy decreases the volume of the stomach and also decreases the parietal cell mass. However, the basic principle of the procedure is similar to that of the biliopancreatic bypass; i.e., producing selective malabsorption by limiting the food digestion and absorption to a short common ileal segment.
- Distal (Long Limb) Gastric Bypass (Roux or alimentary limb > 150 cm
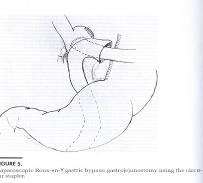
Recently variations of gastric bypass procedures have been described, consisting primarily of long limb Roux-en-Y procedures, which vary in the length of the alimentary and common limbs. For example, the stomach may be divided with a long segment of the jejunum (instead of ileum) anastomosed to the proximal gastric stump, creating the alimentary limb. The remaining pancreaticobiliary limb, consisting of stomach remnant, duodenum, and length of proximal jejunum is then anastomosed to the ileum, creating a common limb of variable length in which the ingested food mixes with the pancreaticobiliary juices. While the long alimentary limb permits absorption of most nutrients, the short common limb primarily limits absorption of fats. The stomach may be bypassed in a variety of ways, either by resection or stapling along the horizontal or vertical axis. Unlike the traditional gastric bypass, which is essentially a gastric restrictive procedure, these very long limb Roux-en-Y gastric bypasses combine gastric restriction with some element of malabsorptive procedure, depending on the location of the anastomoses. . For gastric restrictive procedures, the weight loss is primarily due to reduced caloric intake, and thus the patient must be committed to eating small meals, reinforced by early satiety. For example, gastric restrictive surgery will not be successful in patients who consume high volumes of calorie rich liquids. In patients undergoing biliopancreatic bypass, reduced intake may not be as much of an issue, but patients must adhere to a balanced diet to avoid metabolic complications. In addition, the high potential for metabolic complications requires life-long follow-up. Surgeons need to be adequately trained in the particular techniques and should perform a high volume of these procedures. Laparoscopic Roux --En –Y Gastric Bypass (GBP )- Described in 1994 by Wittgrove.- It is a restrictive procedure with malabsorptive component .- It is the procedure of choice in superobese ,sweet eaters & in patients with GERD
– Technique
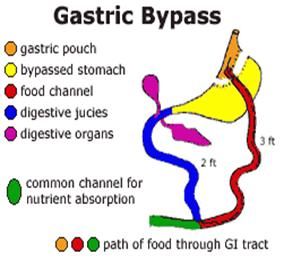
The original gastric bypass surgeries were based on the observation that post-gastrectomy patients tended to lose weight. The current procedure, gastric bypass with horizontal or vertical partition of the stomach in association with a Roux-en-Y procedure (i.e., a gastrojejunal anastomosis). Thus the flow of food bypasses the duodenum and proximal small bowel. The procedure may also be associated with an unpleasant "dumping syndrome," in which a large osmotic load delivered directly to the jejunum from the stomach produces abdominal pain and/or vomiting. The dumping syndrome may further reduce intake, particularly in "sweets eaters. Because the normal flow of food is disrupted, there are more metabolic complications compared to other gastric restrictive procedures, all of which can be corrected by oral supplementation. Another concern is the ability to evaluate the "blind" bypassed portion of the stomach. Gastric bypass may be performed with either an open or laparoscopic technique.



Surgical Complications :
Surgery Early Late
Roux-en-Y gastric bypass Pulmonary embolus Anastomotic stricture Anastomotic leak Marginal ulcer Deep venous thrombosis Gastrointestinal bleeding Gastrointestinal bleeding Dumping syndrome Wound infection Anemia Enterocutaneous fistula Neuropathy-B12 deficiency Small bowel obstruction Dermatitis Sepsis Hair loss Respiratory failure Weight gain Incisional hernia Small bowel obstruction Osteoporosis MalnutritionDuodenal switch Similar to Roux-en-Y gastric bypass Bile salt wasting Diarrhea-secretory Malabsorption Vitamin deficiency DermatitisLaparoscopic adjustable gastric band Gastric prolapse Band erosion Band slippage Port migration Band malposition Port infection Gastric occlusion Disconnection of port tubing Esophageal dilation Malnutrition
Lap. Vertical banded gastroplasty. erosion of the polypropylene mesh enlargement of the pouch, stomal stenosis, reflux esophagitis, mild vitamin deficiencies
Discussion: The criteria of efficacy of any surgey and benefit depend on many factor such as :Weight LossDurability of weight lossShort-term complicationsReoperation RateLong-term complicationsImproved health outcomes in terms of weight-related comorbidities
* Lap. Vertical banded gastroplasty.There are numerous clinical series that report substantial amounts of weight loss following verticalbanded gastroplasty. weight loss of 75% to 100% of excess weight in first one year. But vertical banded gastroplasty has largely been abandoned as longer term, less favorable outcomes have been reported in the literature. While initial results in terms of weight loss, complications and improvement in co morbid conditions were good, these results deteriorated over time . The rate of revision surgery was 29.51% due to inadequate weight loss or complications. Also the procedure was less successful in the super obese patient .*Adjustable Gastric Banding
A major advantage of the LAGB is its safety. also Lower perioperative morbidity and mortality, gradual weight loss with few nutritional complications, and reversibility make LAGB is a good option .LAGB was associated with a median overall morbidity rate of 11.3% with a mean short-term mortality of 0.05%, compared with a 23.6% morbidity and 0.5% mortality for RYGB . Short operative time and hospital stay also is good advantage .
Weight loss after LAGB (especially in sweet eater) is significantly slower than after RYGB, so comparisons between the operations demonstrate superior
weight loss with RYGB . also The need for frequent adjustments is sometimes considered as disadvantage .
The ability to place a band laparoscopically in the massively super obese and in the older morbidly obese patient. offers significant advantages .
Laparoscopic Roux --En –Y Gastric Bypass (GBP )Laparoscopic Roux-en-Y gastric bypass is fast becoming the gold standard for treatment of refractory
morbid obesity. The magnitude of weight loss can be achieved quickly , hospital stay about
3- 4 days, but long operation time ,need good skills and its irriversaple and risk of leak and malabsorption is high .
The Duodenal Switch Operation
The magnitude of weight loss that occurs after the duodenal switch procedure is better than that achieved after the Roux-en-Y gastric bypass procedure.
The mortality and morbidity of the duodenal switch are comparable to other common weight loss procedures, also minimal dietary limitations and metabolic sequelae.also risk of leak is low as compaered RYGB surgey The only limitation is long operation time ,long hospital stay , need good skills and its irriversaple.
Conclusion: 1.Bariatric Surgery is an effective option for sustained w t. Loss in M. O. 2. Long term result from Lap. Bariatric operations should be similar to those of open.3. Lap. Approaches for treatment of M.O. are now available for all bariatric operations.4. Lap. ASGB is emerging as an alternative bariatric surgical option to VBG ,& GBP .5. The criteria used for selecting a patient for a particular operation are still based on surgeon`s experience , training & preference.6. Further studies are required to define subgroups of patients who will benefit from a particular operation.7. The Lap. Malabsorptive procedure is still experimental until further data support it`s safe
References
- BlueCross BlueShield Association Medical Policy Reference Manual, Policy No. 7.01.47
- National Institutes of Health: National Heart, Lung, and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. The Evidence Report. September 1998; No. 98-4083
- Consensus Development Panel. Gastrointestinal surgery for severe obesity. Ann Int Med 1991;115:956-61
- TEC Assessment: Bariatric Surgery for Morbid Obesity, 2003; BlueCross and BlueShield Association Technology Evaluation Center www.bcbs.com/tec/vol18/18_10.html (Verified 12/12/06)
- MacLean LD, Rhode BM, Forse RA. Late results of vertical banded gastroplasty for morbid and super obesity. Surgery 1990;107(1):20-27
- Willbanks OL. Long term results of silicone elastomer ring vertical gastroplasty for the treatment of morbid obesity. Surgery 1987;101(5):606-10
- Brolin RE. Results of obesity surgery. Gastroentrol Clin North Am 1987;16:317-35
- Kolanowski J. Gastroplasty for morbid obesity: The internist's view. Int J Obesity 1995;19(suppl 3):S61-S65
- Melissas J, Christodoulakis M, Spyridakis et al. Disorders associated with clinically severe obesity: significant improvement after surgical weight loss. South Med J 1998;91(12):1143-48
- Hall JC, Watts JM, O'Brien PE, et al. Gastric surgery for morbid obesity. The Adelaide Study. Ann Surg 1990;211(4):419-27
- Sugarman HJ, Starkey JV, Birkenhauer R. A randomized prospective trial of gastric bypass versus vertical banded gastroplasty for morbid obesity and their effects on sweets versus non sweets eaters. Ann Surg 1987;205(6):618-24
- Balsiger BM, Poggio JL, Mai J et al. Ten and more years after vertical banded gastroplasty as primary operation for morbid obesity. J Gastrointest Surg 2000;4(6):598-605
- Arribas del Amos D, Diez M, Gueda M, Diago V. Vertical banded gastroplasty:is it a durable operation for morbid obesity? Obesity Surg 2004;14:536-538
- Griffen WO. Gastric bypass. In: Griffen WO, Printen KJ eds. Surgical management of morbid obesity. New York, NY. Marcel Dekker, Inc, 1987:27-45
- Pories WJ, Swanson MS, MacDonald Kg et al. Who would have thought it? An operation proves to be the most effective therapy for adult onset diabetes mellitus. Ann Surg 1995; 222(3):339-52
- Flickinger EG, Sinar DR, Swanson M. Gastric bypass. Gastroenterol Clin North Am 1987; 16(2):283-92
- Sugarman HJ, Kellum JM, DeMaria EJ. Conversion of proximal to distal gastric bypass for failed gastric bypass for superobesity. J Gastrointest Surg 1997;1:517-25
- Fobi MA, Fleming AW. Vertical banded gastroplasty vs. gastric bypass in the treatment of obesity. J Natl Med Assoc 1988;78(11):1091-98
- TEC Assessment: Laparoscopic Gastric Bypass Surgery for Morbid Obesity, 2005; BlueCross BlueShield Association Technology Evaluation Center www.bcbs.com/tec/vol20/20_15.html (Verified 12/12/06)
- Rutledge R. The mini-gastric bypass: experience with the first 1,274 cases. Obes Surg 2001;11(3):276-8
- Brechner RJ, Farris C, Harrison S, et al. A graded,evidence-based summary of evidence for bariatricsurgery. Surgery of Obesity and Related Diseases2005;1:430–1.
- Oria HE, Carrasquilla C, Cunningham P, et al.Guidelines for weight calculations and follow-up inbariatric surgery. Surgery of Obesity and Related Diseases 2005;1:67–8.
- Nelson LG, Murr M. Operative treatment of clinically significant obesity. Board review series. Hospital Physician 2005;8:2–12.
- National Institutes of Health. Clinical guidelines on the identification, evaluation, and treatment of overweightand obesity in adults: the evidence report. Obes Res 1998;6:51S–209





