Laparoscopic Tubal Sterilization
Laparoscopic sterilization was the first popular minimal access surgical procedure ever performed. Laparoscopic sterilization is a straightforward procedure. Worldwide laparoscopic sterilization is now the most common method used for family planning. Laparoscopic sterilization has evolved by Palmer and Steptoe in the USA by monopolar technique. Rioux and Kleppinger developed a bipolar technique for sterilization because of more cases of bowel injury were reported with the use of monopolar. Later silastic band and spring clips were invented for an occlusive method of sterilization.
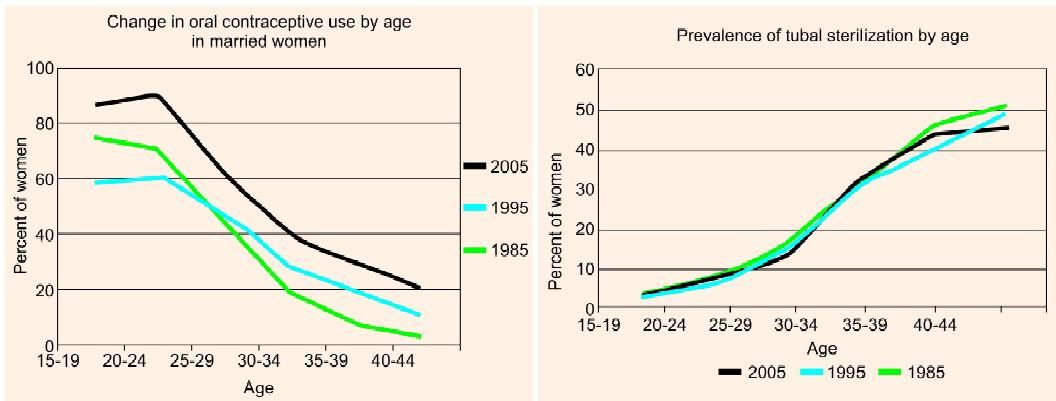
The trend of family planning
Laparoscopic Anatomy
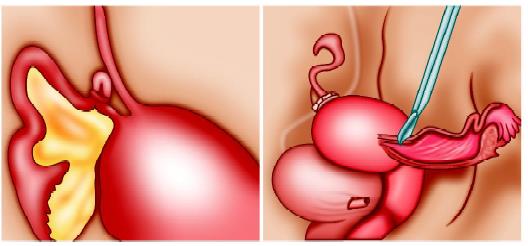
From anterior to posterior, the following important tubular structures are found crossing the brim of the true pelvis: The round ligament of the uterus, the infundibulopelvic ligament, which contains the gonadal vessels and the ureter. The ovaries and fallopian tubes are found between the round ligament and the infundibulopelvic ligament.
The main problem in laparoscopic sterilization surgery is mistaking the round ligament for a fallopian tube. This mistake was more common when single puncture sterilization was used with laparocator. In laprocator the image of the target organ and instrument were in the same axis and this was the cause of more incidence of failure. The next most common mistake is the injury of the ureter during dissection of the infundibulopelvic ligament. If the uterus deviates to the contralateral side with the help of uterine manipulator infundibulopelvic ligament is spread out and a pelvic sidewall triangle is created. The base of this triangle is the round ligament, the medial side is the infundibulopelvic ligament, and the lateral side is the external iliac artery. The apex of this triangle is the point at which the infundibulopelvic ligament crosses the external iliac artery.
Contradictions
• Hemodynamic instability
• Uncorrected coagulopathy
• Severe cardiopulmonary disease
• Abdominal wall infection
• Multiple previous upper abdominal procedures
• Late pregnancy.
Patient Position
The patient should be in steep Trendelenburg and lithotomy position. One assistant should remain between the legs of the patient to do uterine manipulation whenever required.
Port Position
Generally, laparoscopic sterilization is possible with two ports only. Many gynecologists like to perform tube ligation with one port in the umbilicus and other in the suprapubic region. In our practice, we like to put a port in the left iliac fossa. The left iliac fossa port will allow the elevation angle of an instrument at 30° and this angle is better for manipulation of the fallopian tube and good ergonomics.
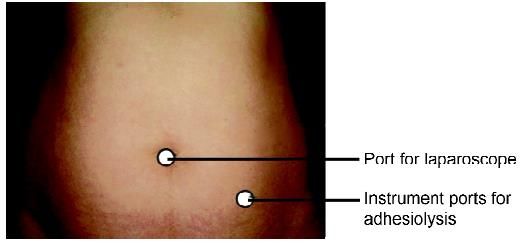
Port position for tubal sterilization
Operative Procedure
Methods of Tubal Sterilization:
• Occlusive
Falope ring and Filshie clip
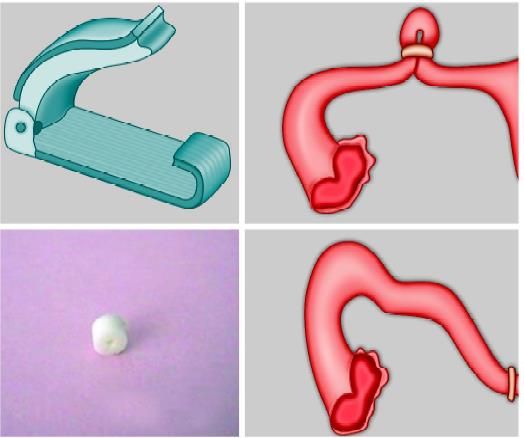
Various occlusive devices for sterilization
Laparoscopic sterilization by an occlusive method is the most popular method of interval sterilization in the USA. The use of laparoscopic sterilization in the immediate postpartum period is not wise and usually planned 4 to 6 weeks after delivery. At the time of postpartum laparoscopic tubal sterilization, there are chances of some complications if performed laparoscopically. At the time of immediate postpartum, the uterus is approximately 20 weeks in size and fills the entire pelvis, rendering insertion of the Veress needle and laparoscopic trocar difficult. Making the sub umbilical mini-laparotomy incision is fast and easy; often it can be performed under regional anesthesia. There is no advantage to performing postpartum tubal sterilization laparoscopically.
Laparoscopic sterilization can be planned together with first trimester MTP but in the second trimester again interval of 6 weeks is essential. The main risk of laparoscopic sterilization just after delivery or after second trimester MTP is because the uterus is large and may be injured by trocar. The occlusion of the tube in the luteal phase may lead to pregnancy just after sterilization. This creates a medicolegal problem for gynecologists. To avoid this problem, a urine pregnancy test should be obtained on the morning of surgery, and the patient should be advised to return for MTP if a sign of intrauterine or ectopic pregnancy develops.
Bipolar Coagulation
Two-port techniques are used for sterilization by electrosurgery. One in the umbilicus and one in the left iliac fossa. Gynecologist stands left to the patient and camera assistant right to the gynecologist. A uterine manipulator is helpful to bring both the tube under vision. The fallopian tube is grasped 2 cm lateral to the uterine end and bipolar is activated. If the tube is coagulated very close to the uterus, there is a chance of development of uteroperitoneal fistula containing endometrial tissue due to the continuous contractility of the uterus. Activation of bipolar should be intermittent and after each activation jaw of bipolar should be slightly opened to avoid sticking of the jaw of bipolar with a tube. The procedure should be repeated in three adjacent areas. If the jaw of bipolar adhered with tube forceps should be gently twisted clockwise and counterclockwise and at the same time the pressure from the handle of grasper is decreased. Some gynecologists prefer coagulation and division of tube between coagulated area but the study has shown that coagulation of 2 to 3 cm of the tube without division is better because division leads to a significant incidence of bleeding from underlying vessels. Bipolar should be applied always at three places. If only one place bipolar coagulation per tube is performed, there is always a risk of spontaneous re-canalization in about three months.
Falope Ring Application
Yoon in 1974, described the Silastic band technique for occlusive tubal sterilization. The Falope ring is applied with the help of Falope ring applicator.
Operative Technique
Sterilization using Falope ring application gained popularity in the 1970s. Initially, the failure rate was high with a single puncture technique using laprocator.
These days a double puncture technique is preferred and has less failure rate compared to a single puncture technique. Pneumoperitoneum is created in the usual manner. First of all diagnostic laparoscopy should be performed to exclude any other abnormality. The Filshie clip or Falope ring is loaded into the receiving edge of the applicator. The clip or ring should be applied across the narrow isthemic area about 2 cm from the cornua. This area is very mobile and easy to see. In the case of the desired re-anastomosis, this area is easy to do anastomosis.
Once the fallopian tube is found the atraumatic grasping forceps are used to pick up one of the tubes, one to two cm lateral to the corneal end of the uterus. The jaw of Falope ring applicator is pushed out and the tube is then drawn into the inner cylinder of Falope ring applicator. Once the Falope ring applicator is fully fired either one or two silicon rubber bands are applied to the grasped segment of the fallopian tube. After the application of the Falope ring, the grasping forceps is moved forward out of the inner cylinder to release the occluded segment of the tube. In a similar manner, the contralateral tube is grasped and the ring is applied. After both the tube is occluded some gynecologists inject indigo carmine dye through the uterus to confirm tubal lumen occlusion. The blenching of the tube after the clip application can also be seen after the successful application of the ring. Blench is due to ischemia and this means that the sterilization is perfect. If everything goes well, the patient can be discharged on the same day. The snapshot pictures and video recording of all the procedure is good practice for future references. Filshie and Hulka clip is also applied in the same manner, the only difference is that clips do not form a loop. Hence, the chances of a reversal of sterilization are better compared to Falope rings.
Laparoscopic sterilization was the first popular minimal access surgical procedure ever performed. Laparoscopic sterilization is a straightforward procedure. Worldwide laparoscopic sterilization is now the most common method used for family planning. Laparoscopic sterilization has evolved by Palmer and Steptoe in the USA by monopolar technique. Rioux and Kleppinger developed a bipolar technique for sterilization because of more cases of bowel injury were reported with the use of monopolar. Later silastic band and spring clips were invented for an occlusive method of sterilization.
The trend of family planning
Laparoscopic Anatomy
From anterior to posterior, the following important tubular structures are found crossing the brim of the true pelvis: The round ligament of the uterus, the infundibulopelvic ligament, which contains the gonadal vessels and the ureter. The ovaries and fallopian tubes are found between the round ligament and the infundibulopelvic ligament.
The main problem in laparoscopic sterilization surgery is mistaking the round ligament for a fallopian tube. This mistake was more common when single puncture sterilization was used with laparocator. In laprocator the image of the target organ and instrument were in the same axis and this was the cause of more incidence of failure. The next most common mistake is the injury of the ureter during dissection of the infundibulopelvic ligament. If the uterus deviates to the contralateral side with the help of uterine manipulator infundibulopelvic ligament is spread out and a pelvic sidewall triangle is created. The base of this triangle is the round ligament, the medial side is the infundibulopelvic ligament, and the lateral side is the external iliac artery. The apex of this triangle is the point at which the infundibulopelvic ligament crosses the external iliac artery.
Contradictions
• Hemodynamic instability
• Uncorrected coagulopathy
• Severe cardiopulmonary disease
• Abdominal wall infection
• Multiple previous upper abdominal procedures
• Late pregnancy.
Patient Position
The patient should be in steep Trendelenburg and lithotomy position. One assistant should remain between the legs of the patient to do uterine manipulation whenever required.
Port Position
Generally, laparoscopic sterilization is possible with two ports only. Many gynecologists like to perform tube ligation with one port in the umbilicus and other in the suprapubic region. In our practice, we like to put a port in the left iliac fossa. The left iliac fossa port will allow the elevation angle of an instrument at 30° and this angle is better for manipulation of the fallopian tube and good ergonomics.
Port position for tubal sterilization
Operative Procedure
Methods of Tubal Sterilization:
- Destructive
- Unipolar
- Bipolar
- Coagulation using thermal cautery
- Ligation and cutting by scissors (Pomeroy technique).
• Occlusive
- Filshie clip
- Falope ring
- Hulka clip.
Falope ring and Filshie clip
Various occlusive devices for sterilization
Laparoscopic sterilization by an occlusive method is the most popular method of interval sterilization in the USA. The use of laparoscopic sterilization in the immediate postpartum period is not wise and usually planned 4 to 6 weeks after delivery. At the time of postpartum laparoscopic tubal sterilization, there are chances of some complications if performed laparoscopically. At the time of immediate postpartum, the uterus is approximately 20 weeks in size and fills the entire pelvis, rendering insertion of the Veress needle and laparoscopic trocar difficult. Making the sub umbilical mini-laparotomy incision is fast and easy; often it can be performed under regional anesthesia. There is no advantage to performing postpartum tubal sterilization laparoscopically.
Laparoscopic sterilization can be planned together with first trimester MTP but in the second trimester again interval of 6 weeks is essential. The main risk of laparoscopic sterilization just after delivery or after second trimester MTP is because the uterus is large and may be injured by trocar. The occlusion of the tube in the luteal phase may lead to pregnancy just after sterilization. This creates a medicolegal problem for gynecologists. To avoid this problem, a urine pregnancy test should be obtained on the morning of surgery, and the patient should be advised to return for MTP if a sign of intrauterine or ectopic pregnancy develops.
Bipolar Coagulation
Two-port techniques are used for sterilization by electrosurgery. One in the umbilicus and one in the left iliac fossa. Gynecologist stands left to the patient and camera assistant right to the gynecologist. A uterine manipulator is helpful to bring both the tube under vision. The fallopian tube is grasped 2 cm lateral to the uterine end and bipolar is activated. If the tube is coagulated very close to the uterus, there is a chance of development of uteroperitoneal fistula containing endometrial tissue due to the continuous contractility of the uterus. Activation of bipolar should be intermittent and after each activation jaw of bipolar should be slightly opened to avoid sticking of the jaw of bipolar with a tube. The procedure should be repeated in three adjacent areas. If the jaw of bipolar adhered with tube forceps should be gently twisted clockwise and counterclockwise and at the same time the pressure from the handle of grasper is decreased. Some gynecologists prefer coagulation and division of tube between coagulated area but the study has shown that coagulation of 2 to 3 cm of the tube without division is better because division leads to a significant incidence of bleeding from underlying vessels. Bipolar should be applied always at three places. If only one place bipolar coagulation per tube is performed, there is always a risk of spontaneous re-canalization in about three months.
Falope Ring Application
Yoon in 1974, described the Silastic band technique for occlusive tubal sterilization. The Falope ring is applied with the help of Falope ring applicator.
Operative Technique
Sterilization using Falope ring application gained popularity in the 1970s. Initially, the failure rate was high with a single puncture technique using laprocator.
These days a double puncture technique is preferred and has less failure rate compared to a single puncture technique. Pneumoperitoneum is created in the usual manner. First of all diagnostic laparoscopy should be performed to exclude any other abnormality. The Filshie clip or Falope ring is loaded into the receiving edge of the applicator. The clip or ring should be applied across the narrow isthemic area about 2 cm from the cornua. This area is very mobile and easy to see. In the case of the desired re-anastomosis, this area is easy to do anastomosis.
Once the fallopian tube is found the atraumatic grasping forceps are used to pick up one of the tubes, one to two cm lateral to the corneal end of the uterus. The jaw of Falope ring applicator is pushed out and the tube is then drawn into the inner cylinder of Falope ring applicator. Once the Falope ring applicator is fully fired either one or two silicon rubber bands are applied to the grasped segment of the fallopian tube. After the application of the Falope ring, the grasping forceps is moved forward out of the inner cylinder to release the occluded segment of the tube. In a similar manner, the contralateral tube is grasped and the ring is applied. After both the tube is occluded some gynecologists inject indigo carmine dye through the uterus to confirm tubal lumen occlusion. The blenching of the tube after the clip application can also be seen after the successful application of the ring. Blench is due to ischemia and this means that the sterilization is perfect. If everything goes well, the patient can be discharged on the same day. The snapshot pictures and video recording of all the procedure is good practice for future references. Filshie and Hulka clip is also applied in the same manner, the only difference is that clips do not form a loop. Hence, the chances of a reversal of sterilization are better compared to Falope rings.





