Complications of Operative Hysteroscopy
• Trauma
– Cervical laceration
– Uterine perforation
– Injury to intra-abdominal viscera-rectum, bladder, intestine.
• Intravasation: Predisposing factors for venous intravasation of distending media:
– Uterine tuberculosis
– Submucous tumor
– Hypoplastic uterus
– Recently traumatized uterine cavity
– Proximal tubal obstruction
– Excessive pressure of instillation
– Infection.
• Exacerbate latent salpingitis
• PID
• Febrile reaction
• Bleeding
• Peritonitis.
Safety Measures
Dilatation of the Cervix
The cervix must be dilated in order to enter the hysteroscope into the uterine cavity. The most resectoscope has an outer sheath diameter of about 9 mm so that cervical dilation using mechanical dilators must be at least this amount. It is optimal to avoid over dilation of the cervix since leakage of the distending media through the cervix and around the hysteroscope (especially under pressures of about 150 mm Hg) then becomes possible.
Some cervical canals are difficult to negotiate with dilators. Different dilators have a variable amount of curvature to choose from. It is possible to perforate the lower uterine segments during dilation. Clinical situations in which perforation is more common include dilation of the pregnant uterus, fibroid uterus, uterus of women exposed to DES in utero, uterus after exposure to prostaglandins for cervical ripening, and infected uterus. Many cases of perforation occur at the onset of dilation and the subsequent dilators then continue to open the perforation site.
Occasionally, a rent in the lower uterine segment occurs during dilation. It is thought that rapid dilation or a difficult dilation involving a stenotic inflexible cervix may enhance the frequency of these tears. It is possible for a tremendous amount of distending media to become intravasated through these rents and into the large vessels of the lower uterine region if they are transacted.
Cervical incompetence following hysteroscopic surgery is rarely reported but theoretically possible. The cervix is composed of a tough fibro connective tissue and smooth muscle. Closure of the internal os of the cervix is the general rule even following manual dilatation of up to 15 mm.
Bleeding
The pressure maintained in the uterine cavity may (but generally should not) exceed both the venous and the arterial pressures so that active blood flow from transacted vessels may not become apparent until the uterus is deflated. At lesser pressures, bleeding can be identified and usually controlled. If there is excessive bleeding following destructive procedures such as endometrial ablation, it can be frequently controlled by tamponade using an inflated Foley catheter balloon (10–30 ml for up to 16 hours) in the uterus. Sometimes the excessive flow can be controlled with estrogens hormonal therapy (if due to denuding the lining).
Excessive Intravasation of Distending Media or CO2 Gas
Whenever vessels are transacted during hysteroscopic surgery and either fluid or gas is entered into the uterine cavity under pressure there is a possibility of intravasation (entry of these substances into the circulation).
D5W (5% Dextrose in water) is a good distending media for diagnostic hysteroscopy. Major complications with this solution are very rare. In fact, there are no reports in the world literature of major morbidity or mortality with the use of D5W at hysteroscopy. Possible complications include water intoxication (a reduction in serum osmolality) with a dilutional reduction in sodium concentration, volume overload (when the circulating volume in the vascular system exceeds the ability of the heart to adequately pump this volume and the excess fluid typically begins to collect in the tissues of the lungs, hypothermia (significant reduction in body temperature) if room temperature solutions are used without warming the patient with devices like a “Bair Hugger” and hyperglycemia (significant excess in circulating glucose concentration that may not be rapidly metabolized if the patient has insulin resistance or diabetes mellitus).
The major complication that most hysteroscopic surgeon’s focus on avoiding is water intoxication. The risk of water intoxication from D5W in a healthy woman with normal renal function is very low since the kidneys can typically produce in excess of 1000 cc of dilute urine in response to a decrease in serum osmolarity.
Adhesions
Following hysteroscopic surgery, there is a chance of adhesion (scar) formation. If significant electrocoagulation is used within the uterine cavity in the infertility patient. Intraoperative estrogen IV (25 or 50 mg of Premarin) and at least a 30-day course of higher dose Premarin postoperatively (1.25 mg or preferably 2.5 mg if tolerated) should be used.
Burn Injury to the Bowel
When resectoscopic electrosurgery is performed in the area of the uterine Ostia (near the entry site of the fallopian tubes) there is a chance of thermal injury to adjacent tissue outside the uterine cavity. This is because the uterine wall in these regions is very thin and heat from the cautery can travel through the uterine wall and burn adjacent bowel.
Infection
Endometritis is uncommon after operative hysteroscopy and antibiotics are usually not “routinely” given. The potential benefits of antibiotics outweigh their risks when exposure to infection occurs.
- Hysteroscopy in Abnormal Uterine Bleeding

Submucous myoma
- Hysteroscopy in Cases of Infertility
- Diagnostic laparoscopy in hysteroscopy

Septate uterus

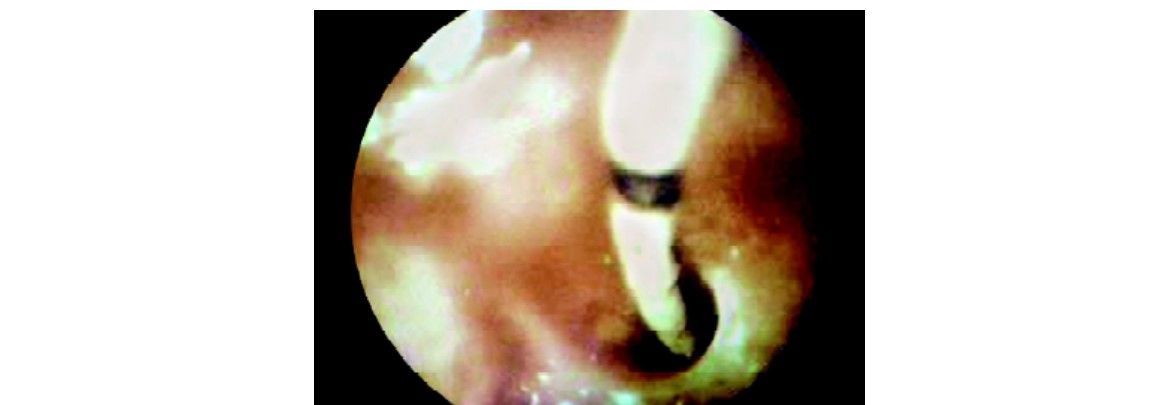
Forgotten IUD
Salpingo-catheterization

Bicornuate uterus
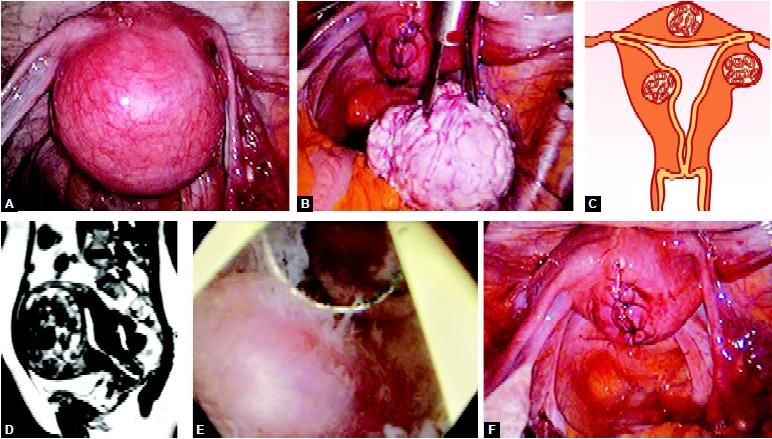
Intramural myoma
Submucous myoma
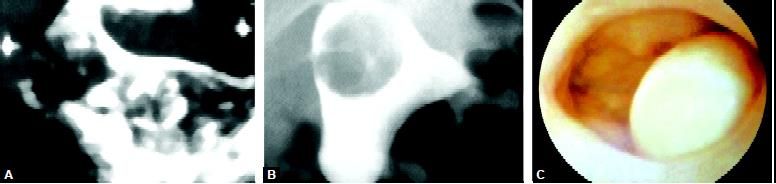
Tubal Cause of Infertility
To clarify the tubal cause of infertility:
The ureteric catheter used to cannulate tube
• Intracavitary pressure rises
• Flow rate falls
• Salpingo-catheterization not possible
• Inability to induce contraction of tubal angle (Post-inflammatory fibrosis)
• Combined laparoscopy and hysteroscopy used for tubal patency tests and therapeutic options.
Hysteroscopic Correlation and Diagnosis
Contraindications of Hysteroscopy
• Absolute
– Adnexal and endometrial infection
• Relative

