Like every surgery laparoscopy features numerous complications including the potential risk of anaesthesia and operation. Although laparoscopis surgery causes less tissue damage then its available counterpart but it's wrong to express that it is totally risk-free operation. Complications of laparoscopy might be categorized according to the various phases of the operation. Problems related to induction from the pneumoperitoneum and insertion of the laparoscope includes cardiac arrhythmias, perforation of a hollow viscus, and puncture of a solid organ, bleeding, and subcutaneous emphysema. In most reported series, complications of laparoscopic surgeries are minor and occur with a frequency of 1-5%, and the mortality rate is approximately 0.05%.
The most popular complications are:
- Additional complications of anaesthesia like cardiac arrhythmia, and respiratory complications.
- Transient high fever.
- Abdominal wall ecchymosis.
- Pneumonia and bronchitis.
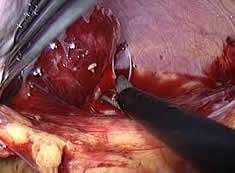
- Bleeding because of injury of unrecognized arteries.
- Problems for internal solid organs.
- Perforation of hollow viscus
- Injury of major arteries.
- Infection.
- Hernia.
- Adhesion formation.
Each one of these complication aren't specific to laparoscopy. These complications are more frequent in available surgery than laparoscopy. Infection is easily the most common complication of any surgical procedure. In laparoscopic surgery rate of infection is extremely under open surgery but many statistical studies shows that infection remains the most typical complication after laparoscopic surgery. This complication is not associated with the laparoscopic technique itself but depends on the sterilization and theater environment from the hospital. The actual Problems for the bowel may be the second most typical reason for morbidity and mortality after laparoscopic surgery. The Problems for bowel and blood vessels is very related to the strategy of laparoscopic surgery. There's a small risk of complications including, problems for the abdominal organs, intestines, urinary bladder or arteries. If the surgeon is not experienced than he can perforate an innocent bowel using the long pointed instruments of laparoscopic surgery. If complication is severe an additional operation are usually necesary with a larger incision to either stop bleeding or repair an injury that cannot be fixed by laparoscopy. In the event of infection along with other mild complication short span of appropriate antibiotic is sufficient to overcome the issue. In experienced hands, complications may occur but aren't frequent. Patient safety ought to be surgeon's strongest concern.
In the event that patient have fever, chills, vomiting, cannot urinate, developed increasing redness at an incision site, or if pain is worsening, distension of abdomen or any discharge in the port site, patient should contact their surgeon promptly. It's a rare complication of minimally invasive surgery due to irritation of peritoneum. Co2 is known to be a peritoneal irritant which produces congestion from the vessels in patients undergoing laparoscopy. An exaggerated response to the irritant may manifest symptoms of weeping peritoneum which is pyrexia, Increased heart rate and respiration cramp abdomen, vomiting and when not treated sometimes leads to severe peritonitis.
Incisional bowel herniation is a complication of operative laparoscopy. Herniations occur through ports 10 mm in dimensions at both umbilical and extra umbilical sites if not closed properly after operation. Surgeons should recognize the importance of shutting fascia at these larger port sites and should maintain a high degree of suspicion in any patient that has a sluggish recovery with intermittent nausea and vomiting after an operative procedure. The underlying fascia and peritoneum should be closed not just when using trocars of 10mm and bigger as previously suggested but additionally when extensive manipulation is conducted through a 5mm trocar port, causing extension from the incision.
Contraindications for laparoscopy are relative and can include the uncooperative patient, uncorrectable coagulation defects, severe congestive heart failure, respiratory insufficiency, suspected acute, diffuse peritonitis, and also the presence of distended bowel. If tense ascites exists, large volume paracentesis can be performed since the preliminary step in the laparoscopy. Previous laparotomy incisions may necessitate alteration from the usual trocar insertion site, or may represent a contraindication towards the procedure. Most surgeons would not recommend laparoscopy in individuals with pre-existing disease conditions. Patients with cardiac diseases and COPD shouldn't be considered a great candidate for laparoscopy. Laparoscopy can also be harder in patients who may have had earlier abdominal surgery. Seniors can also be at increased risk for complications with general anaesthesia coupled with pneumoperitoneum. Laparoscopy does add to the surgical risk in patients with a lower ed cardio-pulmonary reserve regarding the effects of the pneumoperitoneum and a longer operative time.
Preoperative precaution patient should take?
- Affected person should not eat or drink for 6 to 8 hours prior to the procedure.
- Statement of all the investigations ought to be present eg; blood, urine or X-ray testing may be required before your operative procedure.
- Sufferer must have shower the evening before or even the day of your operation. Cleaning of umbilicus with antiseptic soap, water, along with a Q-tip is important.
- Affected individual should report to the hospital in the correct time, which is usually 4-6 hours sooner than your scheduled surgery.
- If affected individual take any medication every day, discuss this with your surgeon as you may have to take some or all of the medication on the day of surgery with a sip of water. For aspirin, blood thinners or arthritis medication, discuss this with your surgeon.
Preoperative precaution patient should consume selecting a surgeon?
The end result of any laparoscopic procedure drastically depends upon the experience of the surgeon. Inside a study from Los Angeles, the outcome of cases operated by generalists were compared with those performed by specialized laparoscopic surgeons. 10 abscesses occurred post operatively within the number of patients whose operation ended by general surgical services when compared with one case within the number of patients whose operation was conducted by expert. Laparoscopy by expert (using skilled dissection, use of retrieval bag, proper ligation of stump and thorough peritoneal toilet) decreases complication rate. In knowledgeable hands, complications may occur but aren't frequent. Patient safety should be your surgeon's strongest concern.




