
Page 64 - World Journal of Laparoscopic Surgeons
P. 64
Abhipsa Mishra, Sujit Behera
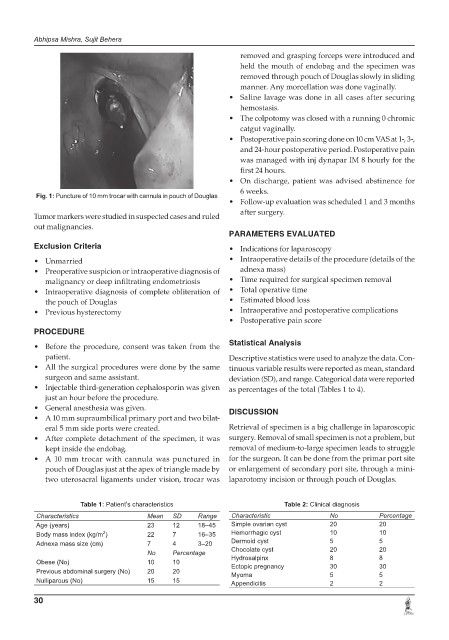
removed and grasping forceps were introduced and
held the mouth of endobag and the specimen was
removed through pouch of Douglas slowly in sliding
manner. Any morcellation was done vaginally.
• Saline lavage was done in all cases after securing
hemostasis.
• The colpotomy was closed with a running 0 chromic
catgut vaginally.
• Postoperative pain scoring done on 10 cm VAS at 1-, 3-,
and 24-hour postoperative period. Postoperative pain
was managed with inj dynapar IM 8 hourly for the
first 24 hours.
• On discharge, patient was advised abstinence for
6 weeks.
Fig. 1: Puncture of 10 mm trocar with cannula in pouch of Douglas
• Follow-up evaluation was scheduled 1 and 3 months
after surgery.
Tumor markers were studied in suspected cases and ruled
out malignancies.
PARAMETERS EVALUATED
Exclusion Criteria • Indications for laparoscopy
• Unmarried • Intraoperative details of the procedure (details of the
• Preoperative suspicion or intraoperative diagnosis of adnexa mass)
malignancy or deep infiltrating endometriosis • Time required for surgical specimen removal
• Intraoperative diagnosis of complete obliteration of • Total operative time
the pouch of Douglas • Estimated blood loss
• Previous hysterectomy • Intraoperative and postoperative complications
• Postoperative pain score
PROCEDURE
• Before the procedure, consent was taken from the Statistical Analysis
patient. Descriptive statistics were used to analyze the data. Con-
• All the surgical procedures were done by the same tinuous variable results were reported as mean, standard
surgeon and same assistant. deviation (SD), and range. Categorical data were reported
• Injectable third-generation cephalosporin was given as percentages of the total (Tables 1 to 4).
just an hour before the procedure.
• General anesthesia was given. DISCUSSION
• A 10 mm supraumbilical primary port and two bilat-
eral 5 mm side ports were created. Retrieval of specimen is a big challenge in laparoscopic
• After complete detachment of the specimen, it was surgery. Removal of small specimen is not a problem, but
kept inside the endobag. removal of medium-to-large specimen leads to struggle
• A 10 mm trocar with cannula was punctured in for the surgeon. It can be done from the primar port site
pouch of Douglas just at the apex of triangle made by or enlargement of secondary port site, through a mini-
two uterosacral ligaments under vision, trocar was laparotomy incision or through pouch of Douglas.
Table 1: Patient’s characteristics Table 2: Clinical diagnosis
Characteristics Mean SD Range Characteristic No Percentage
Age (years) 23 12 18–45 Simple ovarian cyst 20 20
2
Body mass index (kg/m ) 22 7 16–35 Hemorrhagic cyst 10 10
Adnexa mass size (cm) 7 4 3–20 Dermoid cyst 5 5
No Percentage Chocolate cyst 20 20
Obese (No) 10 10 Hydrosalpinx 8 30 8 30
Ectopic pregnancy
Previous abdominal surgery (No) 20 20 Myoma 5 5
Nulliparous (No) 15 15 Appendicitis 2 2
30