
Page 65 - World Journal of Laparoscopic Surgery
P. 65
A Laparoscopic Approach of a Very Large Ovarian Cyst in Young Female
presence of assumed benign cysts has become a gold standard. 9
In the case of laparoscopic surgery treatment depends on several
criteria such as age, menstruation cycle status, size, and structure
of ovarian cyst.
Minimal invasive surgical management for benign ovarian
cysts has become popular nowadays. Various studies demonstrated
a clear advantage of laparoscopy as compared to standard
open surgery in terms of lesser amount of blood loss and
analgesic requirement, better visibility during surgery, minimum
postoperative pain, decreased days of hospital stay, and better
cosmetic outcomes. The person can resume to normal activity
early. 10
During the surgical management of large ovarian cysts in
young girls, the main goal to keep in mind is the preservation of the
reproductive and hormonal function of the ovaries. Frequently cysts
have dense adhesions with the ovary and persevering ipsilateral
ovary could not be possible as encountered in this paper.
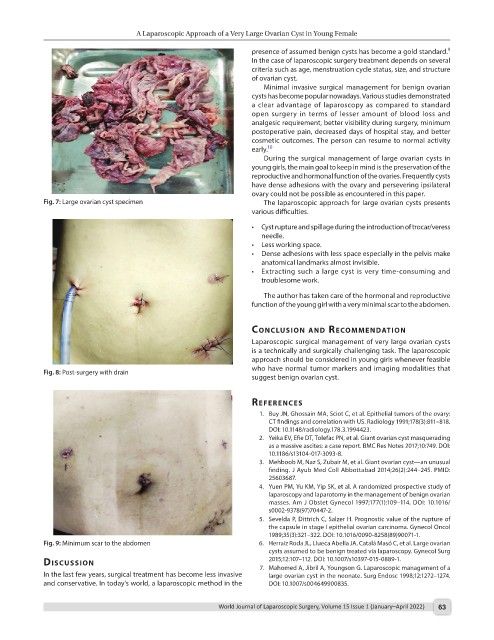
Fig. 7: Large ovarian cyst specimen The laparoscopic approach for large ovarian cysts presents
various difficulties.
• Cyst rupture and spillage during the introduction of trocar/veress
needle.
• Less working space.
• Dense adhesions with less space especially in the pelvis make
anatomical landmarks almost invisible.
• Extracting such a large cyst is very time-consuming and
troublesome work.
The author has taken care of the hormonal and reproductive
function of the young girl with a very minimal scar to the abdomen.
conclusIon And recommendAtIon
Laparoscopic surgical management of very large ovarian cysts
is a technically and surgically challenging task. The laparoscopic
approach should be considered in young girls whenever feasible
who have normal tumor markers and imaging modalities that
Fig. 8: Post-surgery with drain
suggest benign ovarian cyst.
references
1. Buy JN, Ghossain MA, Sciot C, et al. Epithelial tumors of the ovary:
CT findings and correlation with US. Radiology 1991;178(3):811–818.
DOI: 10.1148/radiology.178.3.1994423.
2. Yeika EV, Efie DT, Tolefac PN, et al. Giant ovarian cyst masquerading
as a massive ascites: a case report. BMC Res Notes 2017;10:749. DOI:
10.1186/s13104-017-3093-8.
3. Mehboob M, Naz S, Zubair M, et al. Giant ovarian cyst—an unusual
finding. J Ayub Med Coll Abbottabad 2014;26(2):244–245. PMID:
25603687.
4. Yuen PM, Yu KM, Yip SK, et al. A randomized prospective study of
laparoscopy and laparotomy in the management of benign ovarian
masses. Am J Obstet Gynecol 1997;177(1):109–114. DOI: 10.1016/
s0002-9378(97)70447-2.
5. Sevelda P, Dittrich C, Salzer H. Prognostic value of the rupture of
the capsule in stage I epithelial ovarian carcinoma. Gynecol Oncol
1989;35(3):321–322. DOI: 10.1016/0090-8258(89)90071-1.
Fig. 9: Minimum scar to the abdomen 6. Herraiz Roda JL, Llueca Abella JA, Catalá Masó C, et al. Large ovarian
cysts assumed to be benign treated via laparoscopy. Gynecol Surg
2015;12:107–112. DOI: 10.1007/s10397-015-0889-1.
dIscussIon
7. Mahomed A, Jibril A, Youngson G. Laparoscopic management of a
In the last few years, surgical treatment has become less invasive large ovarian cyst in the neonate. Surg Endosc 1998;12:1272–1274.
and conservative. In today’s world, a laparoscopic method in the DOI: 10.1007/s004649900835.
World Journal of Laparoscopic Surgery, Volume 15 Issue 1 (January–April 2022) 63