
Page 7 - WJOLS
P. 7
Laparoscopic Ultrasound–Guided versus Percutaneous Radiofrequency Ablation in Treatment of Unresectable HCC
Fig. 9: In case of tumors bulging on liver surface, the hilar portion of the tumor was ablated initially in order
to destroy the inflow of blood supplying the tumor
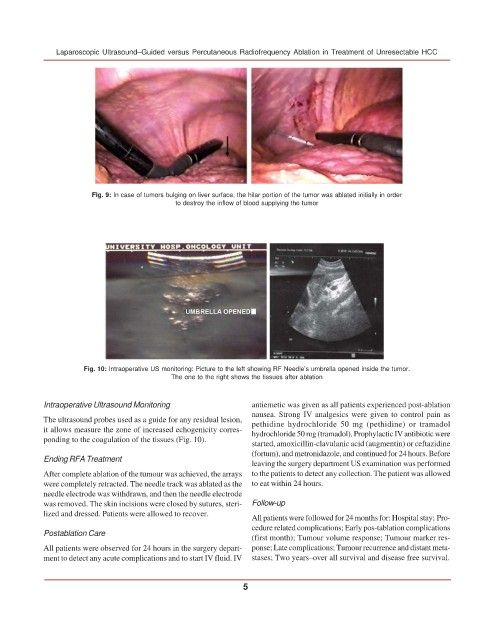
Fig. 10: Intraoperative US monitoring: Picture to the left showing RF Needle’s umbrella opened inside the tumor.
The one to the right shows the tissues after ablation
Intraoperative Ultrasound Monitoring antiemetic was given as all patients experienced post-ablation
nausea. Strong IV analgesics were given to control pain as
The ultrasound probes used as a guide for any residual lesion, pethidine hydrochloride 50 mg (pethidine) or tramadol
it allows measure the zone of increased echogenicity corres- hydrochloride 50 mg (tramadol). Prophylactic IV antibiotic were
ponding to the coagulation of the tissues (Fig. 10).
started, amoxicillin-clavulanic acid (augmentin) or ceftazidine
(fortum), and metronidazole, and continued for 24 hours. Before
Ending RFA Treatment
leaving the surgery department US examination was performed
After complete ablation of the tumour was achieved, the arrays to the patients to detect any collection. The patient was allowed
were completely retracted. The needle track was ablated as the to eat within 24 hours.
needle electrode was withdrawn, and then the needle electrode
was removed. The skin incisions were closed by sutures, steri- Follow-up
lized and dressed. Patients were allowed to recover.
All patients were followed for 24 months for: Hospital stay; Pro-
cedure related complications; Early pos-tablation complications
Postablation Care
(first month); Tumour volume response; Tumour marker res-
All patients were observed for 24 hours in the surgery depart- ponse; Late complications; Tumour recurrence and distant meta-
ment to detect any acute complications and to start IV fluid. IV stases; Two years–over all survival and disease free survival.
5