
Page 5 - World Journal of Laparoscopic Surgery
P. 5
Laparoscopic vs Open Surgical Management of Adhesive Bowel Obstruction in Children
While in open laparotomy group oral feeds were delayed until enterocolitis, appendicectomy for perforated appendix, Meckel’s
day 5–9 (mean = 5.9) and total parenteral nutrition was required diverticulectomy, open surgery for intussusception, various
in many (36) of these cases length of hospital stay in laparoscopic tumors and cyst excisions, and Nissen fundoplication were among
group (range = 3–8 days, mean = 5.5 days) was significantly frequent surgical procedures, which led to the adhesive intestinal
shorter (p ≤ 0.05) than open laparotomy group (range = 6–27 days, obstruction (Fig. 1). Historically, laparotomy with lysis of adhesions
mean = 11.3 days). Thus, over all postoperative recovery was better has been the conventional management for adhesive small bowel
in the laparoscopic group (Table 1). After discharge, all patients were obstruction in children. 18,19 In the adult literature, there have
followed in outpatient department for any symptom or recurrence been multiple retrospective publications demonstrating the
of adhesions for a minimum period of 12 months. Patients operated utility of laparoscopy in the treatment of adhesive small bowel
by open laparotomy follow-up for a period of 12–84 months and obstruction. They show earlier recovery of bowel function and
laparoscopic group patents were followed up from 12 months to reduced length of stay and decreased incisional complications. In
60 months after adhesiolysis. None of the patients in either group addition, laparoscopy has the theoretical advantage of reducing
developed recurrence after surgery. additional adhesion formation and thus recurrence. 20,21 There are
no randomized, controlled trials in the literature that examine the
dIscussIon role of laparoscopy in treating adhesions in children and there are
actually few publications that examine the role of laparoscopy in
In this retrospective study, we reviewed all cases of adhesive the management of adhesions in children. However, recent review
bowel obstruction managed in our department from January articles and case series advocate laparoscopic management of
2007 to September 2017. Nonoperative management was adhesive bowel obstruction in children. 8–10 At our institute, we
started in all children after admission and it was successful in have adopted laparoscopic adhesiolysis since 2012. Our conversion
eight of our cases. Initial conservative management is adopted rate of 10.3% is lower than 23–30% conversion rate reported
in adult and pediatric practice for management of adhesive by other investigators. 8,22–24 All our laparoscopic adhesiolysis
bowel obstruction but the success of conservative treatment in surgeries are performed by an experienced pediatric surgeon
children varies between different studies. 11–14 Certain pediatric who is well versed with advanced laparoscopic skills in children.
surgical procedures like ileostomy closure or formation, Ladd’s We always try to keep laparoscopic adhesiolysis as first case in
procedure for malrotation, appendicectomy for perforated our operation theater in morning hours as far as possible so that
appendix and tumor surgery are more prone to adhesion operating surgeon can work at ease in comfortable environment.
formation. 6,15–17 In our series, ileostomy or colostomy closure after First, trocar is placed by open technique. We lyse adhesion with
anorectal malformation, Hirschsprung’s disease and necrotizing sharp dissection and energy device was used cautiously to divide
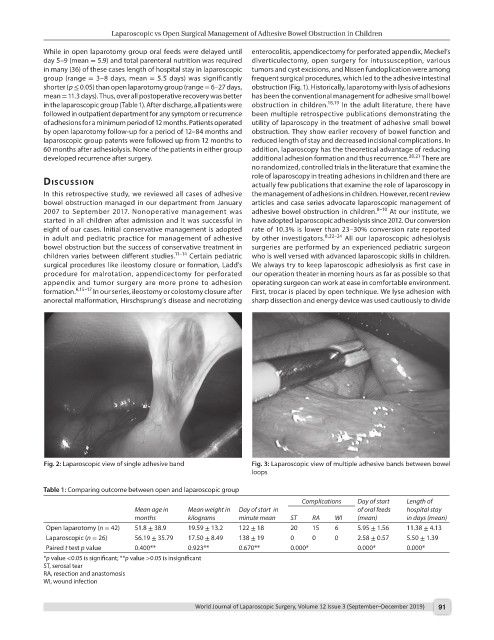
Fig. 2: Laparoscopic view of single adhesive band Fig. 3: Laparoscopic view of multiple adhesive bands between bowel
loops
Table 1: Comparing outcome between open and laparoscopic group
Complications Day of start Length of
Mean age in Mean weight in Day of start in of oral feeds hospital stay
months kilograms minute mean ST RA WI (mean) in days (mean)
Open laparotomy (n = 42) 51.8 ± 38.9 19.59 ± 13.2 122 ± 18 20 15 6 5.95 ± 1.56 11.38 ± 4.13
Laparoscopic (n = 26) 56.19 ± 35.79 17.50 ± 8.49 138 ± 19 0 0 0 2.58 ± 0.57 5.50 ± 1.39
Paired t test p value 0.400** 0.923** 0.670** 0.000* 0.000* 0.000*
*p value <0.05 is significant; **p value >0.05 is insignificant
ST, serosal tear
RA, resection and anastomosis
WI, wound infection
World Journal of Laparoscopic Surgery, Volume 12 Issue 3 (September–December 2019) 91