
Page 17 - World Journal of Laparoscopic Surgery
P. 17
Evaluation of Various Port Positions for Minimal Access Cardiovascular and Thoracic Procedures
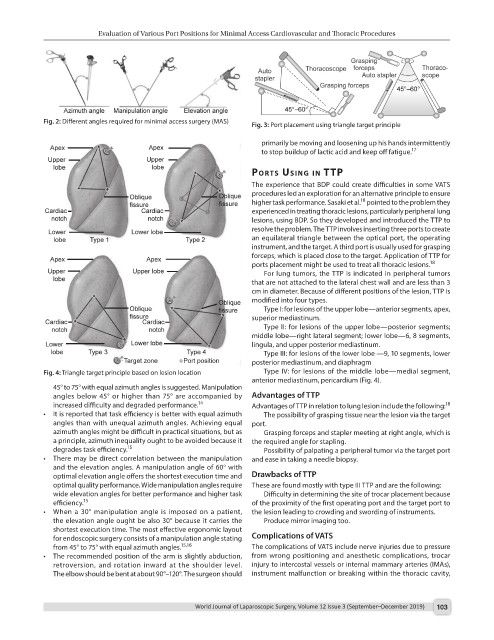
Fig. 2: Different angles required for minimal access surgery (MAS) Fig. 3: Port placement using triangle target principle
primarily be moving and loosening up his hands intermittently
to stop buildup of lactic acid and keep off fatigue. 17
Ports usIng In ttP
The experience that BDP could create difficulties in some VATS
procedures led an exploration for an alternative principle to ensure
18
higher task performance. Sasaki et al. pointed to the problem they
experienced in treating thoracic lesions, particularly peripheral lung
lesions, using BDP. So they developed and introduced the TTP to
resolve the problem. The TTP involves inserting three ports to create
an equilateral triangle between the optical port, the operating
instrument, and the target. A third port is usually used for grasping
forceps, which is placed close to the target. Application of TTP for
ports placement might be used to treat all thoracic lesions. 18
For lung tumors, the TTP is indicated in peripheral tumors
that are not attached to the lateral chest wall and are less than 3
cm in diameter. Because of different positions of the lesion, TTP is
modified into four types.
Type I: for lesions of the upper lobe—anterior segments, apex,
superior mediastinum.
Type II: for lesions of the upper lobe—posterior segments;
middle lobe—right lateral segment; lower lobe—6, 8 segments,
lingula, and upper posterior mediastinum.
Type III: for lesions of the lower lobe —9, 10 segments, lower
posterior mediastinum, and diaphragm
Fig. 4: Triangle target principle based on lesion location Type IV: for lesions of the middle lobe—medial segment,
anterior mediastinum, pericardium (Fig. 4).
45° to 75° with equal azimuth angles is suggested. Manipulation
angles below 45° or higher than 75° are accompanied by Advantages of TTP
increased difficulty and degraded performance. 14 Advantages of TTP in relation to lung lesion include the following: 18
• It is reported that task efficiency is better with equal azimuth The possibility of grasping tissue near the lesion via the target
angles than with unequal azimuth angles. Achieving equal port.
azimuth angles might be difficult in practical situations, but as Grasping forceps and stapler meeting at right angle, which is
a principle, azimuth inequality ought to be avoided because it the required angle for stapling.
degrades task efficiency. 15 Possibility of palpating a peripheral tumor via the target port
• There may be direct correlation between the manipulation and ease in taking a needle biopsy.
and the elevation angles. A manipulation angle of 60° with
optimal elevation angle offers the shortest execution time and Drawbacks of TTP
optimal quality performance. Wide manipulation angles require These are found mostly with type III TTP and are the following:
wide elevation angles for better performance and higher task Difficulty in determining the site of trocar placement because
efficiency. 15 of the proximity of the first operating port and the target port to
• When a 30° manipulation angle is imposed on a patient, the lesion leading to crowding and swording of instruments.
the elevation angle ought be also 30° because it carries the Produce mirror imaging too.
shortest execution time. The most effective ergonomic layout
for endoscopic surgery consists of a manipulation angle stating Complications of VATS
from 45° to 75° with equal azimuth angles. 15,16 The complications of VATS include nerve injuries due to pressure
• The recommended position of the arm is slightly abduction, from wrong positioning and anesthetic complications, trocar
retroversion, and rotation inward at the shoulder level. injury to intercostal vessels or internal mammary arteries (IMAs),
The elbow should be bent at about 90°–120°. The surgeon should instrument malfunction or breaking within the thoracic cavity,
World Journal of Laparoscopic Surgery, Volume 12 Issue 3 (September–December 2019) 103