
Page 35 - World Association of Laparoscopic Surgeons - Journal
P. 35
WJOLS
Prevention of Common Bile Duct Injuries in Laparoscopic Cholecystectomy
removing the gallbladder. It often occurs when the dissection inflammatory mass within which the cystic duct is hidden
is difficult especially or when the gallbladder is intrahepatic. (Figs 2A and B). This visual deception occurs especially in
presence of severe acute or chronic inflammation, a large
Thermal injuries: Cautery induced injuries are also more
stone in the pouch of Hartmann, adhesive bands between
common in the presence of severe inflammation. This is
the gallbladder and the common hepatic duct and
due to the use of excessively high cautery settings to control
intrahepatic gallbladder. Chronic inflammation tends to
hemorrhage.
cause retraction of structures in the porta hepatis, bringing
Tenting injuries: In a tenting injury, the junction of the the gallbladder against the CHD so that it appears as a part
common bile duct and hepatic bile ducts is occluded when of the gallbladder wall. If this view is relied upon for ductal
a clip is placed at the bottom end of the cystic duct while identification it will, in these cases, result in division of the
forcefully pulling up on the gallbladder. CBD. 18
The critical view of safety technique, advocated by
Prevention of Bile Duct Injuries Strasberg involves tentative identification of these cystic
structures by dissection in the triangle of Calot (Figs 3A
Bile duct injury should be regarded as preventable, but in a
and B), followed by dissection of the gallbladder off the
study of surgeons’ anonymous response after bile duct injury
liver bed. In this technique, the triangle of Calot is cleared
during cholecystectomy published in the American Journal
of fat and fibrous tissue and after detachment of the
of Surgery in 2003, over 70% of surgeons regarded it as
unavoidable. 15 Following early experiences with such gallbladder; only two structures are connected to the lower
end of the gallbladder—the cystic duct and artery. It is not
injuries in early 90’s, Hunter and Troidl proposed several
necessary or recommended that the CBD be visualized. 2
techniques to prevent injury: A 30º telescope, avoidance of
Failure to achieve this critical view is an absolute indication
diathermy close to the common hepatic duct, dissection close
for conversion or possibly cholangiography to define ductal
to the gallbladder—cystic duct junction, avoidance of
anatomy.
unnecessary dissection close to the cystic duct—common
Following its introduction, this critical view method has
hepatic duct junction, and conversion to an open approach
been accepted by many surgeons for its superior results with
16,17
when uncertain. However, to apply these techniques,
regards to minimizing BDIs. Averginos et al in 2009
correct interpretation of the anatomy is required.
published the result of 1046 cholecystectomies without BDI
using the critical view method. 20 Only five patients had
Preventing Misidentification Errors
transient biliary leaks in the postoperative period which
Misidentification is due to failure to achieve conclusive
subsided within 2 to 14 days. Similarly, Yegiyants and
identification of the cystic structures. The cystic duct and Collins analyzed the role of critical view of safety in 3,000
artery are the only structures that require division during patients undergoing elective cholecystectomy and reported
cholecystectomy, hence the objective of dissection primarily one bile duct injury, which occurred during dissection of
is to identify these structures conclusively. There are several Calot’s triangle, prior to achieving the critical view. 19,21
methods of identification of the cystic duct. In the open Sanjay et al in 2010 studied its safety in 447 cholecystec-
method, display of the confluence of the cystic duct with tomies done for acute biliary pathologies and reported no
the common hepatic duct to form the common bile duct BDIs. Critical view was obtained in 388 (87%) patients and
was used which is considered not safe in the laparoscopic
method. In the laparoscopic form of surgery, techniques
used are intraoperative cholangiography, the infundibular
technique and the critical view technique.
The infundibular technique is a method initially used
for ductal identification based on three-dimensional
demonstration of the funnel-like shape of the lower end of
the gallbladder and adjacent cystic duct. To obtain this view,
cystic duct is followed onto the gallbladder or the lower
end of the gallbladder is traced down to the cystic duct.
When dissection is completed, the funnel-shaped union of
A B
cystic duct with gallbladder can be seen in three dimensions.
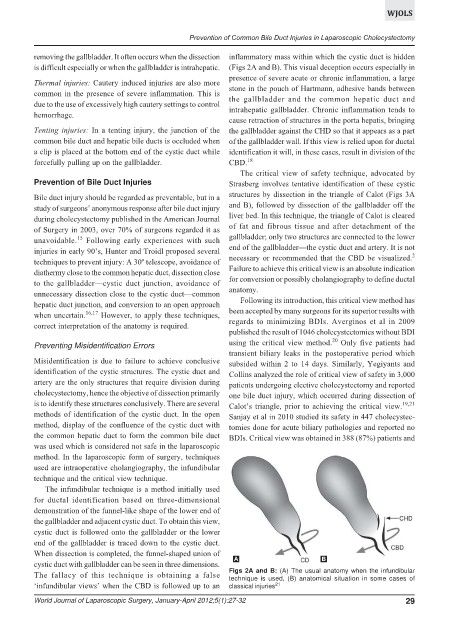
Figs 2A and B: (A) The usual anatomy when the infundibular
The fallacy of this technique is obtaining a false technique is used, (B) anatomical situation in some cases of
‘infundibular views’ when the CBD is followed up to an classical injuries 21
World Journal of Laparoscopic Surgery, January-April 2012;5(1):27-32 29