
Page 4 - Jourmal of World Association of Laparoscopic Surgeon
P. 4
Shailesh Kumar et al
RESULTS Among the 12 patients who developed abdominal wall
emphysema, nine (75%) patients were having BMI > 30.
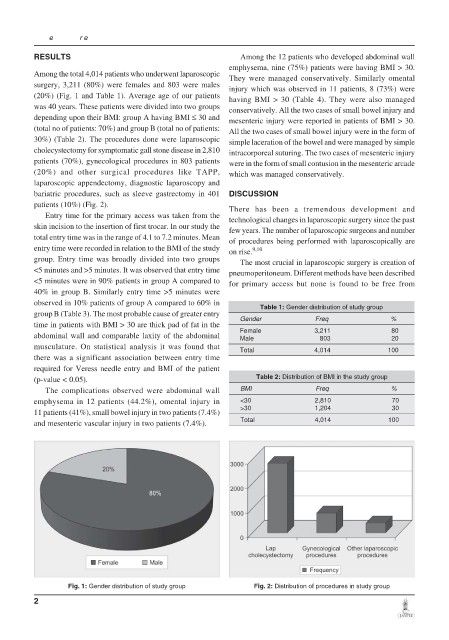
Among the total 4,014 patients who underwent laparoscopic They were managed conservatively. Similarly omental
surgery, 3,211 (80%) were females and 803 were males injury which was observed in 11 patients, 8 (73%) were
(20%) (Fig. 1 and Table 1). Average age of our patients having BMI > 30 (Table 4). They were also managed
was 40 years. These patients were divided into two groups conservatively. All the two cases of small bowel injury and
depending upon their BMI: group A having BMI ≤ 30 and mesenteric injury were reported in patients of BMI > 30.
(total no of patients: 70%) and group B (total no of patients: All the two cases of small bowel injury were in the form of
30%) (Table 2). The procedures done were laparoscopic simple laceration of the bowel and were managed by simple
cholecystectomy for symptomatic gall stone disease in 2,810 intracorporeal suturing. The two cases of mesenteric injury
patients (70%), gynecological procedures in 803 patients were in the form of small contusion in the mesenteric arcade
(20%) and other surgical procedures like TAPP, which was managed conservatively.
laparoscopic appendectomy, diagnostic laparoscopy and
bariatric procedures, such as sleeve gastrectomy in 401 DISCUSSION
patients (10%) (Fig. 2). There has been a tremendous development and
Entry time for the primary access was taken from the technological changes in laparoscopic surgery since the past
skin incision to the insertion of first trocar. In our study the few years. The number of laparoscopic surgeons and number
total entry time was in the range of 4.1 to 7.2 minutes. Mean of procedures being performed with laparoscopically are
entry time were recorded in relation to the BMI of the study on rise. 9,10
group. Entry time was broadly divided into two groups The most crucial in laparoscopic surgery is creation of
<5 minutes and >5 minutes. It was observed that entry time pneumoperitoneum. Different methods have been described
<5 minutes were in 90% patients in group A compared to for primary access but none is found to be free from
40% in group B. Similarly entry time >5 minutes were
observed in 10% patients of group A compared to 60% in Table 1: Gender distribution of study group
group B (Table 3). The most probable cause of greater entry
Gender Freq %
time in patients with BMI > 30 are thick pad of fat in the
abdominal wall and comparable laxity of the abdominal Female 3,211 80
20
803
Male
musculature. On statistical analysis it was found that Total 4,014 100
there was a significant association between entry time
required for Veress needle entry and BMI of the patient
(p-value < 0.05). Table 2: Distribution of BMI in the study group
The complications observed were abdominal wall BMI Freq %
emphysema in 12 patients (44.2%), omental injury in <30 2,810 70
>30 1,204 30
11 patients (41%), small bowel injury in two patients (7.4%)
and mesenteric vascular injury in two patients (7.4%). Total 4,014 100
Fig. 1: Gender distribution of study group Fig. 2: Distribution of procedures in study group
2