
Page 18 - Jourmal of World Association of Laparoscopic Surgeon
P. 18
Bijan Kumar Mukhopadhyay
guesswork or tradition. This approach to suturing has
contributed to a growing concern that the knot construction
employed by many surgeons is not optimal and that they
use faulty technique in tying knots, which is the weakest
link in a tied surgical suture. Important considerations in
wound closure are the type of suture, the tying technique,
and the configuration of the suture loops. When a knotted
suture fails to perform its functions, the consequences may
be disastrous. Massive bleeding may occur when the suture
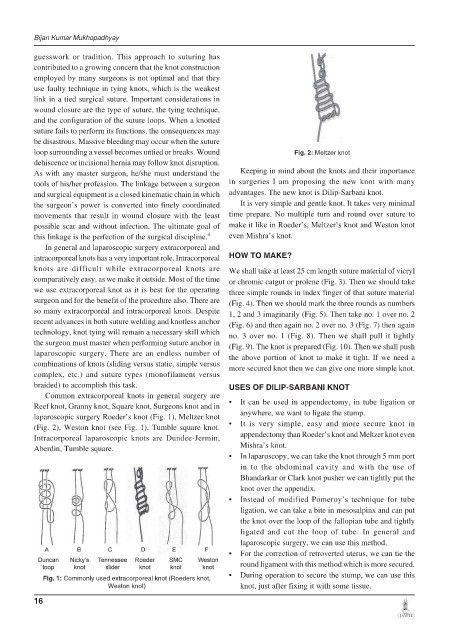
loop surrounding a vessel becomes untied or breaks. Wound Fig. 2: Meltzer knot
dehiscence or incisional hernia may follow knot disruption.
As with any master surgeon, he/she must understand the Keeping in mind about the knots and their importance
tools of his/her profession. The linkage between a surgeon in surgeries I am proposing the new knot with many
and surgical equipment is a closed kinematic chain in which advantages. The new knot is Dilip-Sarbani knot.
the surgeon’s power is converted into finely coordinated It is very simple and gentle knot. It takes very minimal
movements that result in wound closure with the least time prepare. No multiple turn and round over suture to
possible scar and without infection. The ultimate goal of make it like in Roeder’s, Meltzer’s knot and Weston knot
this linkage is the perfection of the surgical discipline. 4 even Mishra’s knot.
In general and laparoscopic surgery extracorporeal and
intracorporeal knots has a very important role. Intracorporeal HOW TO MAKE?
knots are difficult while extracorporeal knots are We shall take at least 25 cm length suture material of vicryl
comparatively easy, as we make it outside. Most of the time or chromic catgut or prolene (Fig. 3). Then we should take
we use extracorporeal knot as it is best for the operating three simple rounds in index finger of that suture material
surgeon and for the benefit of the procedure also. There are (Fig. 4). Then we should mark the three rounds as numbers
so many extracorporeal and intracorporeal knots. Despite 1, 2 and 3 imaginarily (Fig. 5). Then take no. 1 over no. 2
recent advances in both suture welding and knotless anchor (Fig. 6) and then again no. 2 over no. 3 (Fig. 7) then again
technology, knot tying will remain a necessary skill which no. 3 over no. 1 (Fig. 8). Then we shall pull it tightly
the surgeon must master when performing suture anchor in (Fig. 9). The knot is prepared (Fig. 10). Then we shall push
laparoscopic surgery. There are an endless number of the above portion of knot to make it tight. If we need a
combinations of knots (sliding versus static, simple versus more secured knot then we can give one more simple knot.
complex, etc.) and suture types (monofilament versus
braided) to accomplish this task. USES OF DILIP-SARBANI KNOT
Common extracorporeal knots in general surgery are
Reef knot, Granny knot, Square knot, Surgeons knot and in • It can be used in appendectomy, in tube ligation or
laparoscopic surgery Roeder’s knot (Fig. 1), Meltzer knot anywhere, we want to ligate the stump.
(Fig. 2), Weston knot (see Fig. 1), Tumble square knot. • It is very simple, easy and more secure knot in
Intracorporeal laparoscopic knots are Dundee-Jermin, appendectomy than Roeder’s knot and Meltzer knot even
Aberdin, Tumble square. Mishra’s knot.
• In laparoscopy, we can take the knot through 5 mm port
in to the abdominal cavity and with the use of
Bhandarkar or Clark knot pusher we can tightly put the
knot over the appendix.
• Instead of modified Pomeroy’s technique for tube
ligation, we can take a bite in mesosalpinx and can put
the knot over the loop of the fallopian tube and tightly
ligated and cut the loop of tube. In general and
laparoscopic surgery, we can use this method.
• For the correction of retroverted uterus, we can tie the
round ligament with this method which is more secured.
Fig. 1: Commonly used extracorporeal knot (Roeders knot, • During operation to secure the stump, we can use this
Weston knot) knot, just after fixing it with some tissue.
16