
Page 40 - WJOLS
P. 40
Bashir Yunusa et al
Fig. 16: picture of manipulation angle Fig. 19: Laparoscopic surgical team of the investigator
the higher it approaches nonreproducibility due to fatigue
from increased elevation angle and shoulder overstretching.
This is in keeping with the Baseball Diamond concepts of
port positioning.
ConCLUSIon
There is no ‘ideal port position in urological laparoscopic
procedures based on anatomical landmarks, but the closer
the ports’ positions are to make a manipulation angle of 60º
(Baseball Diamond), the closer to ideal it will be.
RECoMMEndATIonS
More work is to be done on the newly emerging laparo s
Fig. 17: ports’ positions copic urology particularly in the developing world.
REFEREnCES
1. Supe AN, Kulkarni GV, Supe PA. Ergonomics in laparoscopic
surgery. J Min Access Surg 2010;6:31-36.
2. Karthik S, Augustine AJ, Shibumon MM, Pai MV. Analysis of
laparoscopic port site complications: a descriptive study. J Min
Access Surg 2013;9:59-64.
3. Greberg CF, Gettman MT. Instrumentation for natural orifice
transluminal endoscopic surgery and laparoendoscopic single
site surgery. Ind J Urol 2010;26:385-388.
4. Gupta NP, Gautam G. Laparoscopic nephrectomy for benign
nonfunctioning kidneys. J Min Access Surg 2005;149154.
5. Maurya K, Sivanandam SE, Sukumar S, Bhat S, Kumar G,
Nair B. Concomitant laparoscopic urological procedures: does
it contribute to morbidity? J Min Access Surg 2009;5:67-71.
6. World Laparoscopy Hospital. Cyberciti, DLF Phase II, NCR
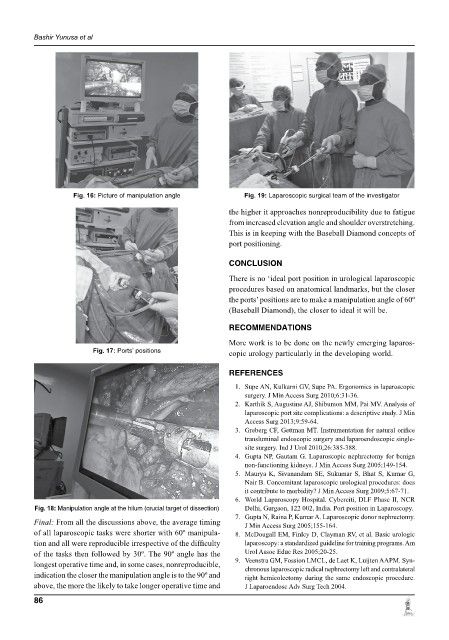
Fig. 18: manipulation angle at the hilum (crucial target of dissection) Delhi, Gurgaon, 122 002, India. Port position in Laparoscopy.
7. Gupta N, Raina P, Kumar A. Laparoscopic donor nephrectomy.
Final: From all the discussions above, the average timing J Min Access Surg 2005;155164.
of all laparoscopic tasks were shorter with 60º manipula 8. McDougall EM, Finley D, Clayman RV, et al. Basic urologic
tion and all were reproducible irrespective of the difficulty laparoscopy: a standardized guideline for training programs. Am
of the tasks then followed by 30º. The 90º angle has the Urol Assoc Educ Res 2005;20-25.
longest operative time and, in some cases, nonreproducible, 9. Veenstra GM, Fossion LMCL, de Laet K, Luijten AAPM. Syn
chronous laparoscopic radical nephrectomy left and contralateral
indication the closer the manipulation angle is to the 90º and right hemicolectomy during the same endoscopic procedure.
above, the more the likely to take longer operative time and J Laparoendosc Adv Surg Tech 2004.
86