
Page 39 - World Journal of Laparoscopic Surgery
P. 39
WJOLS
Hysteroscopy in Uterine Anomalies: An Edge
first period after her surgery and has been regularly apart (Figs 1E and 3). A hysteroscopic metroplasty
menstruating since then, much to her and her fam- was done and both cavities were enlarged. Lower
ily’s joy. Follow-up ultrasonography (USG) was done, half of the uterine cavities were unified by cutting
which interestingly showed her ovaries’ size to be the adjoining myometrial tissues of both the horns
larger and normal than before and a uterus of size using a traditional monopolar resectoscope. After
66 × 40 × 27 mm. Endometrium now was being well the procedure the uterine horns on laparoscopy had
formed and typically triple layered. come closer. An intrauterine device (after removing
2. A 40-year-old nulliparous lady complaining of chronic copper) was inserted and she was put on sequential
pelvic pain and severe dysmenorrhea for the past few hormones. Her 2nd look surgery gave a perfectly
years worsened over the past few months. She was normal healed cavity (Fig. 1F).
also concerned about her future fertility options. 4. A 33-year-old female came with a complaint of pain
Ultrasonography showed a unicornuate uterus with in lower abdomen, with history of secondary infer-
a left-sided uterine horn with an endometrial cavity; tility and two miscarriages, diagnosed as complete
these findings were confirmed by MRI (Figs 1C and 2). uterine septum with two cervices (bicollis) (Fig. 1G).
The patient underwent diagnostic and operative A diagnostic and operative laparoscopy and hysteros-
hysteroscopy with lateral meteroplasty, while diag- copy was advised. Hysteroscopic septal resection was
nostic and operative laparoscopy with resection of performed with resectoscope by keeping both cervices
the rudimentary horn and fulguration of endome- intact under general anesthesia in early proliferative
triotic lesions. The findings on hysteroscopy were phase (Fig. 1H). She conceived and delivered a term
unicornuate small uterine cavity, with right-side ostia healthy baby girl by lower segment cesarean section.
visualized. All four walls were normal; cervical canal Intraoperatively, uterus was normal and no septum
also normal; on laparoscopy unicornuate uterus with was seen.
left-sided noncommunicating rudimentary horn with 5. A 26-year-old with history of (h/o) two miscarriages
an endometrial cavity was seen; B/L tubes normal; came as a case of secondary infertility. She had two
B/L ovaries: Endometriotic spots seen. Endometriotic spontaneous abortions at 8 and 9 weeks. Her hystero-
spots were seen on the utero-sacral ligaments and salpingography (HSG) revealed partial uterine sep-
bowel adherent to left pelvic wall. At the end, the tum and B/L tubes patent with free spillage (Fig. 1I).
cavity was much larger and adequate for conception Ultrasound showed bicornuate uterus. Thus a diag-
(Fig. 1D). nostic and operative laparoscopy and hysteroscopy
3. A case of 25-year-old lady with history of one sponta- was advised. Hysteroscopic septoplasty was per-
neous abortion at 14 weeks, 2 years earlier. Now anx- formed with scissors, and intrauterine device was
ious to conceive. On hysteroscopy both cornua in the inserted after removing copper coil (Figs 1J and 4).
lower half were close together, simulating a septate or On laparoscopy, uterus was normal in size with
bicornuate uterus. In the upper part, they were further broad fundus. Her relook hysteroscopy a month later
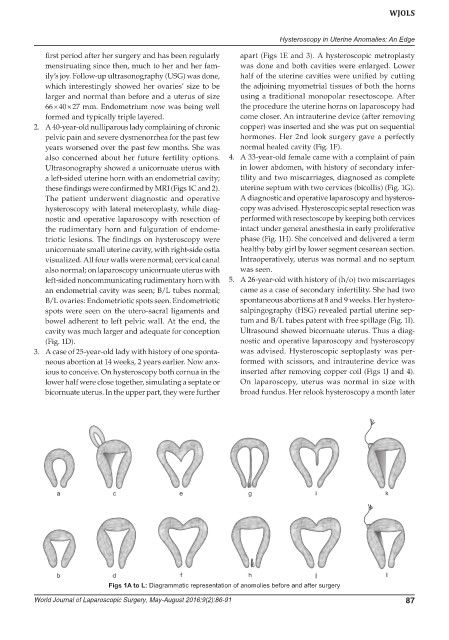
Figs 1A to L: Diagrammatic representation of anomolies before and after surgery
World Journal of Laparoscopic Surgery, May-August 2016;9(2):86-91 87