
Page 12 - World Journal of Laparoscopic Surgery
P. 12
Ahmed E Lasheen et al
E F
G H
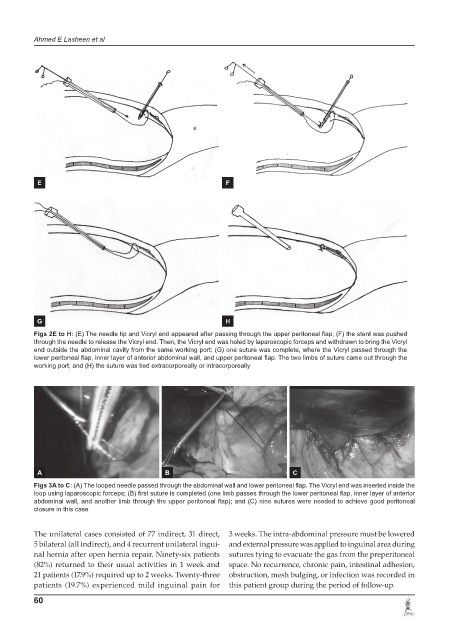
Figs 2E to H: (E) The needle tip and Vicryl end appeared after passing through the upper peritoneal flap; (F) the stent was pushed
through the needle to release the Vicryl end. Then, the Vicryl end was holed by laparoscopic forceps and withdrawn to bring the Vicryl
end outside the abdominal cavity from the same working port; (G) one suture was complete, where the Vicryl passed through the
lower peritoneal flap, inner layer of anterior abdominal wall, and upper peritoneal flap. The two limbs of suture came out through the
working port; and (H) the suture was tied extracorporeally or intracorporeally
A B C
Figs 3A to C: (A) The looped needle passed through the abdominal wall and lower peritoneal flap. The Vicryl end was inserted inside the
loop using laparoscopic forceps; (B) first suture is completed (one limb passes through the lower peritoneal flap, inner layer of anterior
abdominal wall, and another limb through the upper peritoneal flap); and (C) nine sutures were needed to achieve good peritoneal
closure in this case
The unilateral cases consisted of 77 indirect, 31 direct, 3 weeks. The intra-abdominal pressure must be lowered
5 bilateral (all indirect), and 4 recurrent unilateral ingui- and external pressure was applied to inguinal area during
nal hernia after open hernia repair. Ninety-six patients sutures tying to evacuate the gas from the preperitoneal
(82%) returned to their usual activities in 1 week and space. No recurrence, chronic pain, intestinal adhesion,
21 patients (17.9%) required up to 2 weeks. Twenty-three obstruction, mesh bulging, or infection was recorded in
patients (19.7%) experienced mild inguinal pain for this patient group during the period of follow-up.
60