
Page 55 - World Journal of Laparoscopic Surgery
P. 55
Laparoscopic Ventral Hernia Repair
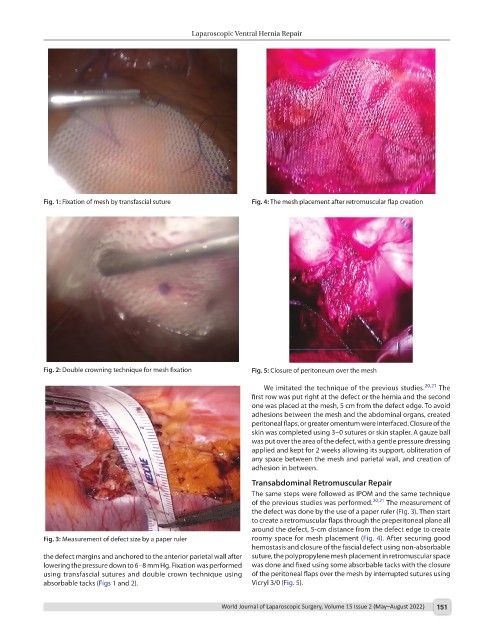
Fig. 1: Fixation of mesh by transfascial suture Fig. 4: The mesh placement after retromuscular flap creation
Fig. 2: Double crowning technique for mesh fixation Fig. 5: Closure of peritoneum over the mesh
We imitated the technique of the previous studies. 20,21 The
first row was put right at the defect or the hernia and the second
one was placed at the mesh, 5 cm from the defect edge. To avoid
adhesions between the mesh and the abdominal organs, created
peritoneal flaps, or greater omentum were interfaced. Closure of the
skin was completed using 3–0 sutures or skin stapler. A gauze ball
was put over the area of the defect, with a gentle pressure dressing
applied and kept for 2 weeks allowing its support, obliteration of
any space between the mesh and parietal wall, and creation of
adhesion in between.
Transabdominal Retromuscular Repair
The same steps were followed as IPOM and the same technique
of the previous studies was performed. 20,21 The measurement of
the defect was done by the use of a paper ruler (Fig. 3). Then start
to create a retromuscular flaps through the preperitoneal plane all
around the defect, 5-cm distance from the defect edge to create
Fig. 3: Measurement of defect size by a paper ruler roomy space for mesh placement (Fig. 4). After securing good
hemostasis and closure of the fascial defect using non-absorbable
the defect margins and anchored to the anterior parietal wall after suture, the polypropylene mesh placement in retromuscular space
lowering the pressure down to 6–8 mm Hg. Fixation was performed was done and fixed using some absorbable tacks with the closure
using transfascial sutures and double crown technique using of the peritoneal flaps over the mesh by interrupted sutures using
absorbable tacks (Figs 1 and 2). Vicryl 3/0 (Fig. 5).
World Journal of Laparoscopic Surgery, Volume 15 Issue 2 (May–August 2022) 151