
Page 56 - World Journal of Laparoscopic Surgery
P. 56
Laparoscopic Ventral Hernia Repair
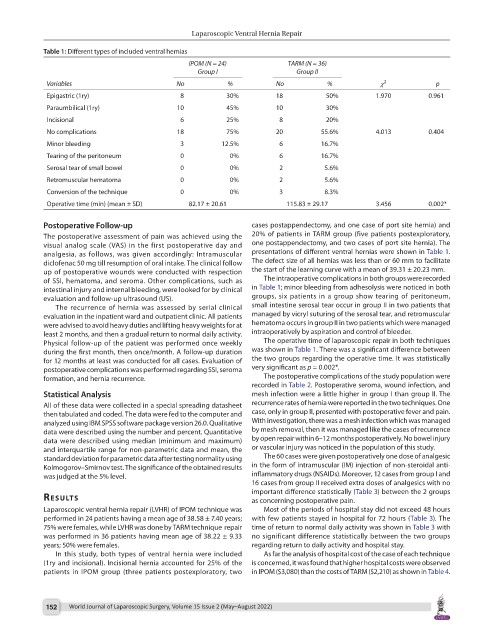
Table 1: Different types of included ventral hernias
IPOM (N = 24) TARM (N = 36)
Group I Group II
Variables No % No % χ 2 p
Epigastric (1ry) 8 30% 18 50% 1.970 0.961
Paraumbilical (1ry) 10 45% 10 30%
Incisional 6 25% 8 20%
No complications 18 75% 20 55.6% 4.013 0.404
Minor bleeding 3 12.5% 6 16.7%
Tearing of the peritoneum 0 0% 6 16.7%
Serosal tear of small bowel 0 0% 2 5.6%
Retromuscular hematoma 0 0% 2 5.6%
Conversion of the technique 0 0% 3 8.3%
Operative time (min) (mean ± SD) 82.17 ± 20.61 115.83 ± 29.17 3.456 0.002*
Postoperative Follow-up cases postappendectomy, and one case of port site hernia) and
The postoperative assessment of pain was achieved using the 20% of patients in TARM group (five patients postexploratory,
visual analog scale (VAS) in the first postoperative day and one postappendectomy, and two cases of port site hernia). The
analgesia, as follows, was given accordingly: Intramuscular presentations of different ventral hernias were shown in Table 1.
diclofenac 50 mg till resumption of oral intake. The clinical follow The defect size of all hernias was less than or 60 mm to facilitate
up of postoperative wounds were conducted with respection the start of the learning curve with a mean of 39.31 ± 20.23 mm.
of SSI, hematoma, and seroma. Other complications, such as The intraoperative complications in both groups were recorded
intestinal injury and internal bleeding, were looked for by clinical in Table 1; minor bleeding from adhesolysis were noticed in both
evaluation and follow-up ultrasound (US). groups, six patients in a group show tearing of peritoneum,
The recurrence of hernia was assessed by serial clinical small intestine serosal tear occur in group II in two patients that
evaluation in the inpatient ward and outpatient clinic. All patients managed by vicryl suturing of the serosal tear, and retromuscular
were advised to avoid heavy duties and lifting heavy weights for at hematoma occurs in group II in two patients which were managed
least 2 months, and then a gradual return to normal daily activity. intraoperatively by aspiration and control of bleeder.
Physical follow-up of the patient was performed once weekly The operative time of laparoscopic repair in both techniques
during the first month, then once/month. A follow-up duration was shown in Table 1. There was a significant difference between
for 12 months at least was conducted for all cases. Evaluation of the two groups regarding the operative time. It was statistically
postoperative complications was performed regarding SSI, seroma very significant as p = 0.002*.
formation, and hernia recurrence. The postoperative complications of the study population were
recorded in Table 2. Postoperative seroma, wound infection, and
Statistical Analysis mesh infection were a little higher in group I than group II. The
All of these data were collected in a special spreading datasheet recurrence rates of hernia were reported in the two techniques. One
then tabulated and coded. The data were fed to the computer and case, only in group II, presented with postoperative fever and pain.
analyzed using IBM SPSS software package version 26.0. Qualitative With investigation, there was a mesh infection which was managed
data were described using the number and percent. Quantitative by mesh removal, then it was managed like the cases of recurrence
data were described using median (minimum and maximum) by open repair within 6–12 months postoperatively. No bowel injury
and interquartile range for non-parametric data and mean, the or vascular injury was noticed in the population of this study.
standard deviation for parametric data after testing normality using The 60 cases were given postoperatively one dose of analgesic
Kolmogorov–Smirnov test. The significance of the obtained results in the form of intramuscular (IM) injection of non-steroidal anti-
was judged at the 5% level. inflammatory drugs (NSAIDs). Moreover, 12 cases from group I and
16 cases from group II received extra doses of analgesics with no
important difference statistically (Table 3) between the 2 groups
results as concerning postoperative pain.
Laparoscopic ventral hernia repair (LVHR) of IPOM technique was Most of the periods of hospital stay did not exceed 48 hours
performed in 24 patients having a mean age of 38.58 ± 7.40 years; with few patients stayed in hospital for 72 hours (Table 3). The
75% were females, while LVHR was done by TARM technique repair time of return to normal daily activity was shown in Table 3 with
was performed in 36 patients having mean age of 38.22 ± 9.33 no significant difference statistically between the two groups
years; 50% were females. regarding return to daily activity and hospital stay.
In this study, both types of ventral hernia were included As far the analysis of hospital cost of the case of each technique
(1ry and incisional). Incisional hernia accounted for 25% of the is concerned, it was found that higher hospital costs were observed
patients in IPOM group (three patients postexploratory, two in IPOM ($3,080) than the costs of TARM ($2,210) as shown in Table 4.
152 World Journal of Laparoscopic Surgery, Volume 15 Issue 2 (May–August 2022)