
Page 7 - WJOLS - Surgery Journal
P. 7
Amnioscopy Revival as a Fetal Surveillance Tool
pregnancy with no predefined risk factor were recruited into appropriate for gestational age. The randomization sequence
the study. All women signed consent forms before participation. placed 47 patients in the A-group, 15 in the B-group and 18 in
Pregnant women with premature rupture of membranes, fetal the C-group. Table 1 illustrates that maternal demographics
anomaly, closed cervix, unexplained vaginal bleeding and active were equivalent between the groups. 7(8.75%) of the 80 patients
labor were excluded. Patient information, demographics, and experienced intrauterine growth restriction that all of them were
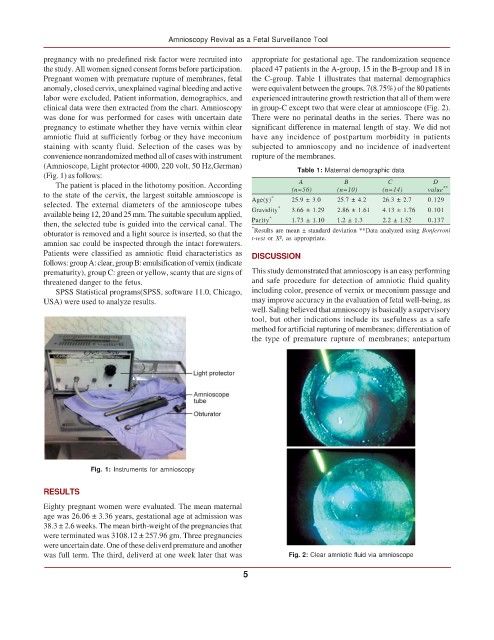
clinical data were then extracted from the chart. Amnioscopy in group-C except two that were clear at amnioscope (Fig. 2).
was done for was performed for cases with uncertain date There were no perinatal deaths in the series. There was no
pregnancy to estimate whether they have vernix within clear significant difference in maternal length of stay. We did not
amniotic fluid at sufficiently forbag or they have meconium have any incidence of postpartum morbidity in patients
staining with scanty fluid. Selection of the cases was by subjected to amnioscopy and no incidence of inadvertent
convenience nonrandomized method all of cases with instrument rupture of the membranes.
(Amnioscope, Light protector 4000, 220 volt, 50 Hz,German) Table 1: Maternal demographic data
(Fig. 1) as follows:
The patient is placed in the lithotomy position. According A B C D **
to the state of the cervix, the largest suitable amnioscope is * (n=56) (n=10) (n=14) value
selected. The external diameters of the amnioscope tubes Age(y) * 25.9 ± 3.0 25.7 ± 4.2 26.3 ± 2.7 0.129
available being 12, 20 and 25 mm. The suitable speculum applied, Gravidity 3.66 ± 1.29 2.86 ± 1.61 4.13 ± 1.76 0.101
*
then, the selected tube is guided into the cervical canal. The Parity 1.73 ± 1.10 1.2 ± 1.3 2.2 ± 1.52 0.137
* Results are mean ± standard deviation **Data analyzed using Bonferroni
obturator is removed and a light source is inserted, so that the t-test or X², as appropriate.
amnion sac could be inspected through the intact forewaters.
Patients were classified as amniotic fluid characteristics as DISCUSSION
follows: group A: clear, group B: emulsification of vernix (indicate
prematurity), group C: green or yellow, scanty that are signs of This study demonstrated that amnioscopy is an easy performing
threatened danger to the fetus. and safe procedure for detection of amniotic fluid quality
SPSS Statistical programs(SPSS, software 11.0, Chicago, including color, presence of vernix or meconium passage and
USA) were used to analyze results. may improve accuracy in the evaluation of fetal well-being, as
well. Saling believed that amnioscopy is basically a supervisory
tool, but other indications include its usefulness as a safe
method for artificial rupturing of membranes; differentiation of
the type of premature rupture of membranes; antepartum
Fig. 1: Instruments for amnioscopy
RESULTS
Eighty pregnant women were evaluated. The mean maternal
age was 26.06 ± 3.36 years, gestational age at admission was
38.3 ± 2.6 weeks. The mean birth-weight of the pregnancies that
were terminated was 3108.12 ± 257.96 gm. Three pregnancies
were uncertain date. One of these deliverd premature and another
was full term. The third, deliverd at one week later that was Fig. 2: Clear amniotic fluid via amnioscope
5