
Page 37 - Journal of WALS
P. 37
Sagar Basanale
Fig. 2: Dissection, opening of peritoneum, initial vascular approach, Fig. 3: Extra-abdominal preparation for proximal segment
mobilization of sigmoid colon EndoGIA-type mechanical suturing device
anastomosis was made in all cases under laparoscopic control,
and a low-pressure aspirative drain was placed next to the
anastomosis. Protective ileostomy was performed in cases with
very low anastomoses and in patients who had undergone
previous neoadjuvant treatment, although this was always done
at the discretion of the surgeon. Conversion was defined as the
need to carry out an unplanned incision or an incision of greater
than normal size to complete the dissection and/or section of
the distal end of the rectum. A Pfannenstiel incision or
infraumbilical middle laparotomy was performed at the discretion
of the surgeon (Fig. 3).
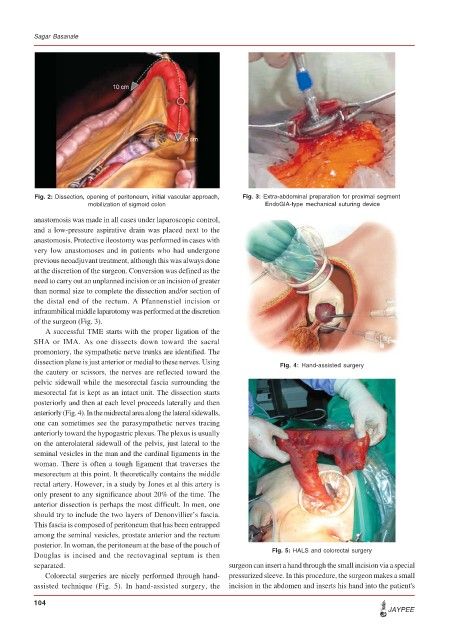
A successful TME starts with the proper ligation of the
SHA or IMA. As one dissects down toward the sacral
promontory, the sympathetic nerve trunks are identified. The
dissection plane is just anterior or medial to these nerves. Using Fig. 4: Hand-assisted surgery
the cautery or scissors, the nerves are reflected toward the
pelvic sidewall while the mesorectal fascia surrounding the
mesorectal fat is kept as an intact unit. The dissection starts
posteriorly and then at each level proceeds laterally and then
anteriorly (Fig. 4). In the midrectal area along the lateral sidewalls,
one can sometimes see the parasympathetic nerves tracing
anteriorly toward the hypogastric plexus. The plexus is usually
on the anterolateral sidewall of the pelvis, just lateral to the
seminal vesicles in the man and the cardinal ligaments in the
woman. There is often a tough ligament that traverses the
mesorectum at this point. It theoretically contains the middle
rectal artery. However, in a study by Jones et al this artery is
only present to any significance about 20% of the time. The
anterior dissection is perhaps the most difficult. In men, one
should try to include the two layers of Denonvillier’s fascia.
This fascia is composed of peritoneum that has been entrapped
among the seminal vesicles, prostate anterior and the rectum
posterior. In woman, the peritoneum at the base of the pouch of
Douglas is incised and the rectovaginal septum is then Fig. 5: HALS and colorectal surgery
separated. surgeon can insert a hand through the small incision via a special
Colorectal surgeries are nicely performed through hand- pressurized sleeve. In this procedure, the surgeon makes a small
assisted technique (Fig. 5). In hand-assisted surgery, the incision in the abdomen and inserts his hand into the patient's
104
JAYPEE