
Page 20 - Journal of WALS
P. 20
Puneet K Kochhar, Pranay Ghosh
used with flexible fibers. However, they are more endometriotic implants does not affect all factors by which
expensive. endometriosis contributes to infertility. 23
29
The best therapy is performed with the CO laser Adamson in 1997 proposed that surgery for endometriosis-
2
vaporization in association with an accurate dissection associated infertility is more effective for severe than mild
technique. 7 endometriosis.
• Tissue response electrosurgical generator (Ligasure™):
This has unique vessel sealing ability. It can be used on Adhesions
vessels up to 7 mm. It precisely confines its effects to the Adhesiolysis is difficult in cases of endometriosis. Adhesions
target tissue with virtually no charring, and with minimal are thick and vascular, and often involve bowel, broad ligament,
thermal spread to adjacent tissue. It senses body’s collagen tubes, etc. Different techniques can be employed individually
to actually change the nature of the vessel walls by or in association. The best method involves dissection with
obliterating the lumen. forceps and/or dissectors, and aquadissection in conjunction
with a CO laser (in place of scissors) (Figs 2 and 3).
2
ENDOSCOPIC SURGERY IN ENDOMETRIOSIS-
ASSOCIATED INFERTILITY Endometriomas
Endometriotic Implants There are two different surgical techniques to treat the
The destruction of implants can be achieved using numerous endometrioma:
techniques: Precise excision, bipolar coagulation, monopolar i. Cystectomy with excision of the endometriotic cyst (Fig. 4)
coagulation, CO laser vaporization or excision, and different ii. Drainage/aspiration of the cyst content and ablation of the
2
methods of coagulation using other types of laser. Superficial cyst capsule with laser or electrocoagulation (Figs 5 and 6).
peritoneal endometriosis is vaporized with the laser, coagulated
with monopolar or bipolar current or excised. Implants less than Cystectomy
2 mm can be coagulated, vaporized or excised. When lesion is Any periovarian adhesions must be removed prior to
greater than 3 mm, vaporization or excision is needed. Lesions cystectomy. An entry site is made in the endometrioma on the
15
greater than 5 mm must be excised or deeply vaporized (Fig. 1). opposite side of the ovarian hilus. The endometrioma is
Current guidelines for the treatment of stages I and II evacuated and repeatedly washed. A ‘cystoscopy’ is then
endometriosis-associated infertility recommend ablation of performed by introducing the laparoscope into the
endometriosis lesions plus adhesiolysis to improve fertility. 25,26 endometriotic cavity. The inner lining of the cyst is examined to
The beneficial effect of surgical removal of the lesions in mild confirm the diagnosis and to eliminate the presence of a
27
endometriosis is small and may be short-lived. This may be malignant cyst. A forceps is used to grasp the ovary at the
due to the fact that a number of occult lesions may be left edge of the incision. A second pair of grasping forceps holds
behind after removal of the visible lesions. These may develop the lining of the cyst. Then, by applying countertraction to the
into minimal endometriosis and grow further. two forceps, cleavage is performed. Generally, the best approach
Thus, the optimal time for conception is within the first is to pull the cyst away from the ovary.
28
18 months following surgical resection. However, even after When the cyst has been completely cleaved, it must be
surgery, the monthly fecundity rate remains lower than that in removed from the abdomen using an ‘endoscopy bag’ or
fertile women. This suggests that the destruction of visible through a suprapubic trocar or the umbilical trocar. A thorough
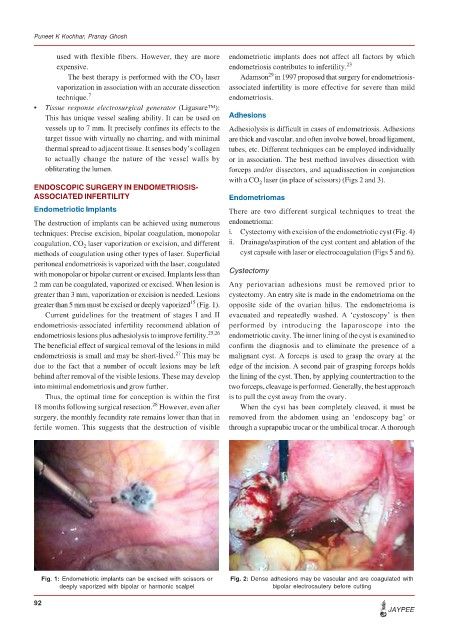
Fig. 1: Endometriotic implants can be excised with scissors or Fig. 2: Dense adhesions may be vascular and are coagulated with
deeply vaporized with bipolar or harmonic scalpel bipolar electrocautery before cutting
92
JAYPEE