
Page 47 - Jourmal of World Association of Laparoscopic Surgeon
P. 47
WJOLS
Two Trocar Laparoscopic Repair of Morgagni Hernia in Infant and Childhood: Simplified Technique
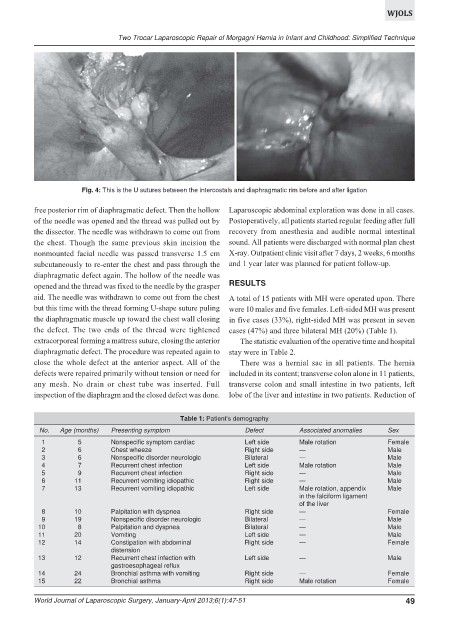
Fig. 4: This is the U sutures between the intercostals and diaphragmatic rim before and after ligation
free posterior rim of diaphragmatic defect. Then the hollow Laparoscopic abdominal exploration was done in all cases.
of the needle was opened and the thread was pulled out by Postoperatively, all patients started regular feeding after full
the dissector. The needle was withdrawn to come out from recovery from anesthesia and audible normal intestinal
the chest. Though the same previous skin incision the sound. All patients were discharged with normal plan chest
nonmounted facial needle was passed transverse 1.5 cm X-ray. Outpatient clinic visit after 7 days, 2 weeks, 6 months
subcutaneously to re-enter the chest and pass through the and 1 year later was planned for patient follow-up.
diaphragmatic defect again. The hollow of the needle was
opened and the thread was fixed to the needle by the grasper RESULTS
aid. The needle was withdrawn to come out from the chest A total of 15 patients with MH were operated upon. There
but this time with the thread forming U-shape suture puling were 10 males and five females. Left-sided MH was present
the diaphragmatic muscle up toward the chest wall closing in five cases (33%), right-sided MH was present in seven
the defect. The two ends of the thread were tightened cases (47%) and three bilateral MH (20%) (Table 1).
extracorporeal forming a mattress suture, closing the anterior The statistic evaluation of the operative time and hospital
diaphragmatic defect. The procedure was repeated again to stay were in Table 2.
close the whole defect at the anterior aspect. All of the There was a hernial sac in all patients. The hernia
defects were repaired primarily without tension or need for included in its content; transverse colon alone in 11 patients,
any mesh. No drain or chest tube was inserted. Full transverse colon and small intestine in two patients, left
inspection of the diaphragm and the closed defect was done. lobe of the liver and intestine in two patients. Reduction of
Table 1: Patient’s demography
No. Age (months) Presenting symptom Defect Associated anomalies Sex
1 5 Nonspecific symptom cardiac Left side Male rotation Female
2 6 Chest wheeze Right side — Male
3 6 Nonspecific disorder neurologic Bilateral — Male
4 7 Recurrent chest infection Left side Male rotation Male
5 9 Recurrent chest infection Right side — Male
6 11 Recurrent vomiting idiopathic Right side — Male
7 13 Recurrent vomiting idiopathic Left side Male rotation, appendix Male
in the falciform ligament
of the liver
8 10 Palpitation with dyspnea Right side — Female
9 19 Nonspecific disorder neurologic Bilateral — Male
10 8 Palpitation and dyspnea Bilateral — Male
11 20 Vomiting Left side — Male
12 14 Constipation with abdominal Right side — Female
distension
13 12 Recurrent chest infection with Left side — Male
gastroesophageal reflux
14 24 Bronchial asthma with vomiting Right side — Female
15 22 Bronchial asthma Right side Male rotation Female
World Journal of Laparoscopic Surgery, January-April 2013;6(1):47-51 49