
Page 20 - Laparoscopic Surgery Online Journal
P. 20
Manash Ranjan Sahoo et al
OPERATIVE TECHNIQUE circular stapler passed per anally (Figs 3 and 4). For LAR,
temporary diverting covering loop ileostomy is used
Patient was placed in head down Lloyd-Davies
(Fig. 5).
Trendelenburg position with surgeon and camera assistant
In patients with APR, pelvic dissection done as far
on patient’s right side. Five ports were routinely used with
distally as possible abdomen opened by extension of port
subumbilical port used for 30º angled telescope. No
in left lower quadrant, descending colon transected
deviation from basic principles of open oncologic colorectal
extracorporeally and end colostomy created. Conventional
surgery was permitted and performed as follows:
perineal dissection and delivery of specimen through
laparoscopic abdominal exploration, preliminary
perineal wound. Perineal drains routinely used. Throughout
identification, ligation and transection of IMA (Fig. 1) and
the surgery meticulous hemostasis was maintained to prevent
IMV with clips, mobilization of left hemicolon and splenic
light absorption by hemoglobin which reduces picture
flexure, identification of ureters and hypogastric nerves
quality.
bilaterally, rectal mobilization (for higher lesion mesorectal
tissue down to 5 cm below tumor routinely excised and TME RESULTS
in tumors of middle and distal third) and intracorporeal The patients characteristics in laparoscopic or open resection
transection of rectum below growth with an endoluminal group are summarized in Table 1. The two groups were
stapler (Fig. 2) in case of restorative resection. Abdomen comparable in terms of age, sex, American Society of
opened by Pfannenstiel incision (maximum 5 cm length) Anesthesia score (ASA score), pathologic stage and type
and resection of tumor bearing bowel completed extra- of resection.
corporeally. Anvil of circular stapler inserted into proximal The mean operating time was significantly longer in LAP
bowel, gut put back in peritoneal cavity, pneumoperitoneum resection group than in open resection group. The amount
re-established and intracorporeal anastomosis done with of operative blood loss was lower in LAP resection group
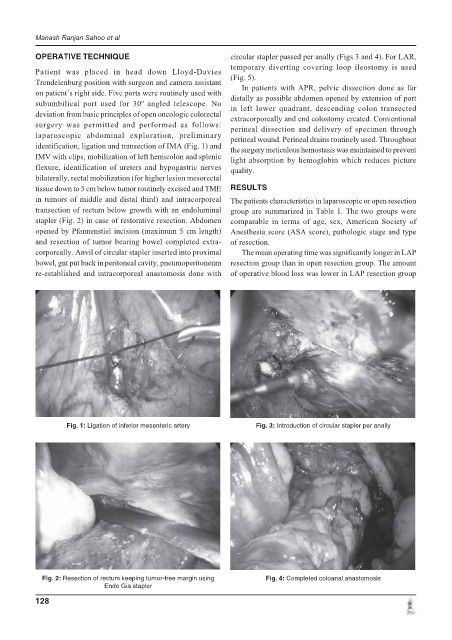
Fig. 1: Ligation of inferior mesenteric artery Fig. 3: Introduction of circular stapler per anally
Fig. 2: Resection of rectum keeping tumor-free margin using Fig. 4: Completed coloanal anastomosis
Endo Gia stapler
128