
Page 22 - Journal of Laparoscopic Surgery
P. 22
Sumanta Kumar Ghosh
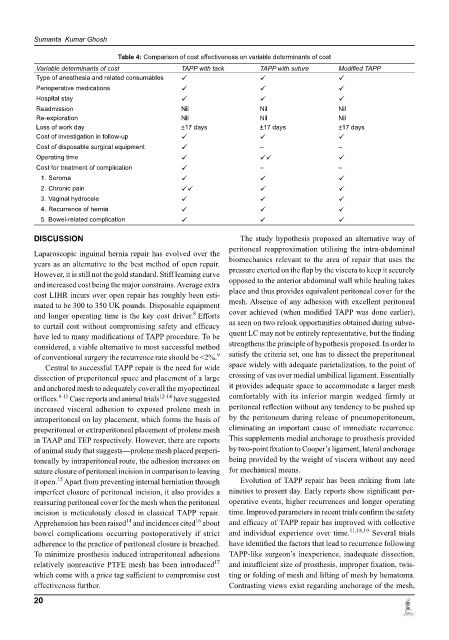
Table 4: Comparison of cost effectiveness on variable determinants of cost
Variable determinants of cost TAPP with tack TAPP with suture Modified TAPP
Type of anesthesia and related consumables
Perioperative medications
Hospital stay
Readmission Nil Nil Nil
Re-exploration Nil Nil Nil
Loss of work day ±17 days ±17 days ±17 days
Cost of investigation in follow-up
Cost of disposable surgical equipment – –
Operating time
Cost for treatment of complication – –
1. Seroma
2. Chronic pain
3. Vaginal hydrocele
4. Recurrence of hernia
5. Bowel-related complication
dISCuSSIon The study hypothesis proposed an alternative way of
peritoneal reapproximation utilising the intra-abdominal
Laparoscopic inguinal hernia repair has evolved over the
years as an alternative to the best method of open repair. biomechanics relevant to the area of repair that uses the
However, it is still not the gold standard. Stiff learning curve pressure exerted on the flap by the viscera to keep it securely
and increased cost being the major constrains. Average extra opposed to the anterior abdominal wall while healing takes
cost LIHR incurs over open repair has roughly been esti- place and thus provides equivalent peritoneal cover for the
mated to be 300 to 350 UK pounds. Disposable equipment mesh. Absence of any adhesion with excellent peritoneal
8
and longer operating time is the key cost driver. Efforts cover achieved (when modified TAPP was done earlier),
to curtail cost without compromising safety and efficacy as seen on two relook opportunities obtained during subse-
have led to many modifications of TAPP procedure. To be quent LC may not be entirely representative, but the finding
considered, a viable alternative to most successful method strengthens the principle of hypothesis proposed. In order to
of conventional surgery the recurrence rate should be <2%. 9 satisfy the criteria set, one has to dissect the preperitoneal
Central to successful TAPP repair is the need for wide space widely with adequate parietalization, to the point of
dissection of preperitoneal space and placement of a large crossing of vas over medial umbilical ligament. Essentially
and anchored mesh to adequately cover all the myopectineal it provides adequate space to accommodate a larger mesh
orifices. 9-11 Case reports and animal trials 12-14 have suggested comfortably with its inferior margin wedged firmly at
increased visceral adhesion to exposed prolene mesh in peritoneal reflection without any tendency to be pushed up
intraperitoneal on lay placement, which forms the basis of by the peritoneum during release of pneumoperitoneum,
preperitoneal or extraperitoneal placement of prolene mesh eliminating an important cause of immediate recurrence.
in TAAP and TEP respectively. However, there are reports This supplements medial anchorage to prosthesis provided
of animal study that suggests—prolene mesh placed preperi- by two-point fixation to Cooper’s ligament, lateral anchorage
toneally by intraperitoneal route, the adhesion increases on being provided by the weight of viscera without any need
suture closure of peritoneal incision in comparison to leaving for mechanical means.
15
it open. Apart from preventing internal herniation through Evolution of TAPP repair has been striking from late
imperfect closure of peritoneal incision, it also provides a nineties to present day. Early reports show significant per-
reassuring peritoneal cover for the mesh when the peritoneal operative events, higher recurrences and longer operating
incision is meticulously closed in classical TAPP repair. time. Improved parameters in recent trials confirm the safety
14
Apprehension has been raised and incidences cited about and efficacy of TAPP repair has improved with collective
16
bowel complications occurring postoperatively if strict and individual experience over time. 11,18,19 Several trials
adherence to the practice of peritoneal closure is breached. have identified the factors that lead to recurrence following
To minimize prosthesis induced intraperitoneal adhesions TAPP-like surgeon’s inexperience, inadequate dissection,
17
relatively nonreactive PTFE mesh has been introduced and insufficient size of prosthesis, improper fixation, twis-
which come with a price tag sufficient to compromise cost ting or folding of mesh and lifting of mesh by hematoma.
effectiveness further. Contrasting views exist regarding anchorage of the mesh,
20