
Page 87 - World Journal of Laparoscopic Surgery
P. 87
Laparoscopic Reversal of Hartmann’s Procedure
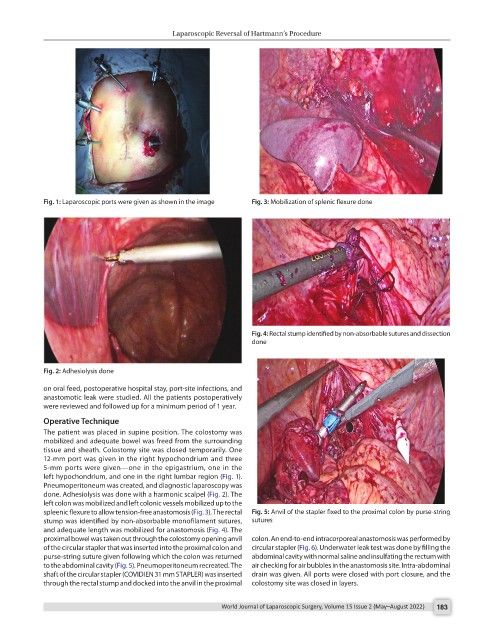
Fig. 1: Laparoscopic ports were given as shown in the image Fig. 3: Mobilization of splenic flexure done
Fig. 4: Rectal stump identified by non-absorbable sutures and dissection
done
Fig. 2: Adhesiolysis done
on oral feed, postoperative hospital stay, port-site infections, and
anastomotic leak were studied. All the patients postoperatively
were reviewed and followed up for a minimum period of 1 year.
Operative Technique
The patient was placed in supine position. The colostomy was
mobilized and adequate bowel was freed from the surrounding
tissue and sheath. Colostomy site was closed temporarily. One
12-mm port was given in the right hypochondrium and three
5-mm ports were given—one in the epigastrium, one in the
left hypochondrium, and one in the right lumbar region (Fig. 1).
Pneumoperitoneum was created, and diagnostic laparoscopy was
done. Adhesiolysis was done with a harmonic scalpel (Fig. 2). The
left colon was mobilized and left colonic vessels mobilized up to the
spleenic flexure to allow tension-free anastomosis (Fig. 3). The rectal Fig. 5: Anvil of the stapler fixed to the proximal colon by purse-string
stump was identified by non-absorbable monofilament sutures, sutures
and adequate length was mobilized for anastomosis (Fig. 4). The
proximal bowel was taken out through the colostomy opening anvil colon. An end-to-end intracorporeal anastomosis was performed by
of the circular stapler that was inserted into the proximal colon and circular stapler (Fig. 6). Underwater leak test was done by filling the
purse-string suture given following which the colon was returned abdominal cavity with normal saline and insulfating the rectum with
to the abdominal cavity (Fig. 5). Pneumoperitoneum recreated. The air checking for air bubbles in the anastomosis site. Intra-abdominal
shaft of the circular stapler (COVIDIEN 31 mm STAPLER) was inserted drain was given. All ports were closed with port closure, and the
through the rectal stump and docked into the anvil in the proximal colostomy site was closed in layers.
World Journal of Laparoscopic Surgery, Volume 15 Issue 2 (May–August 2022) 183