
Page 79 - World Journal of Laparoscopic Surgery
P. 79
Impacted Esophageal Denture with Esophageal Perforation
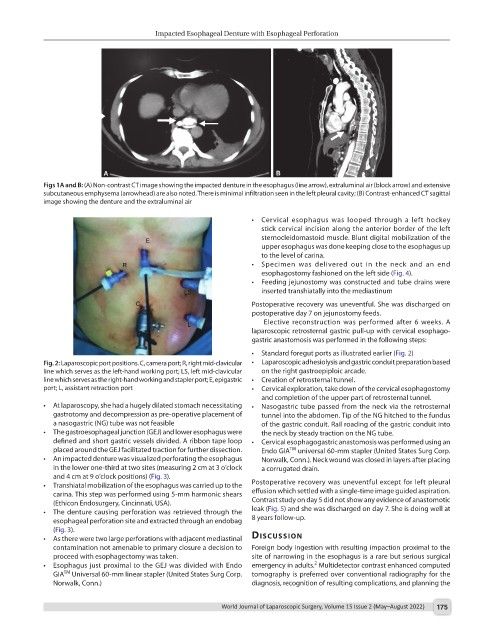
Figs 1A and B: (A) Non-contrast CT image showing the impacted denture in the esophagus (line arrow), extraluminal air (block arrow) and extensive
subcutaneous emphysema (arrowhead) are also noted. There is minimal infiltration seen in the left pleural cavity; (B) Contrast-enhanced CT sagittal
image showing the denture and the extraluminal air
• Cervical esophagus was looped through a left hockey
stick cervical incision along the anterior border of the left
sternocleidomastoid muscle. Blunt digital mobilization of the
upper esophagus was done keeping close to the esophagus up
to the level of carina.
• Specimen was delivered out in the neck and an end
esophagostomy fashioned on the left side (Fig. 4).
• Feeding jejunostomy was constructed and tube drains were
inserted transhiatally into the mediastinum
Postoperative recovery was uneventful. She was discharged on
postoperative day 7 on jejunostomy feeds.
Elective reconstruction was performed after 6 weeks. A
laparoscopic retrosternal gastric pull-up with cervical esophago-
gastric anastomosis was performed in the following steps:
• Standard foregut ports as illustrated earlier (Fig. 2)
Fig. 2: Laparoscopic port positions. C, camera port; R, right mid-clavicular • Laparoscopic adhesiolysis and gastric conduit preparation based
line which serves as the left-hand working port; LS, left mid-clavicular on the right gastroepiploic arcade.
line which serves as the right-hand working and stapler port; E, epigastric • Creation of retrosternal tunnel.
port; L, assistant retraction port • Cervical exploration, take down of the cervical esophagostomy
and completion of the upper part of retrosternal tunnel.
• At laparoscopy, she had a hugely dilated stomach necessitating • Nasogastric tube passed from the neck via the retrosternal
gastrotomy and decompression as pre-operative placement of tunnel into the abdomen. Tip of the NG hitched to the fundus
a nasogastric (NG) tube was not feasible of the gastric conduit. Rail roading of the gastric conduit into
• The gastroesophageal junction (GEJ) and lower esophagus were the neck by steady traction on the NG tube.
defined and short gastric vessels divided. A ribbon tape loop • Cervical esophagogastric anastomosis was performed using an
placed around the GEJ facilitated traction for further dissection. Endo GIA universal 60-mm stapler (United States Surg Corp.
TM
• An impacted denture was visualized perforating the esophagus Norwalk, Conn.). Neck wound was closed in layers after placing
in the lower one-third at two sites (measuring 2 cm at 3 o’clock a corrugated drain.
and 4 cm at 9 o’clock positions) (Fig. 3).
• Transhiatal mobilization of the esophagus was carried up to the Postoperative recovery was uneventful except for left pleural
carina. This step was performed using 5-mm harmonic shears effusion which settled with a single-time image guided aspiration.
(Ethicon Endosurgery, Cincinnati, USA). Contrast study on day 5 did not show any evidence of anastomotic
• The denture causing perforation was retrieved through the leak (Fig. 5) and she was discharged on day 7. She is doing well at
esophageal perforation site and extracted through an endobag 8 years follow-up.
(Fig. 3).
• As there were two large perforations with adjacent mediastinal dIscussIon
contamination not amenable to primary closure a decision to Foreign body ingestion with resulting impaction proximal to the
proceed with esophagectomy was taken. site of narrowing in the esophagus is a rare but serious surgical
2
• Esophagus just proximal to the GEJ was divided with Endo emergency in adults. Multidetector contrast enhanced computed
TM
GIA Universal 60-mm linear stapler (United States Surg Corp. tomography is preferred over conventional radiography for the
Norwalk, Conn.) diagnosis, recognition of resulting complications, and planning the
World Journal of Laparoscopic Surgery, Volume 15 Issue 2 (May–August 2022) 175