
Page 28 - Journal of WALS
P. 28
WJOLS
Risk of Pneumoperitoneum in Obese: Old Myths and New Realities
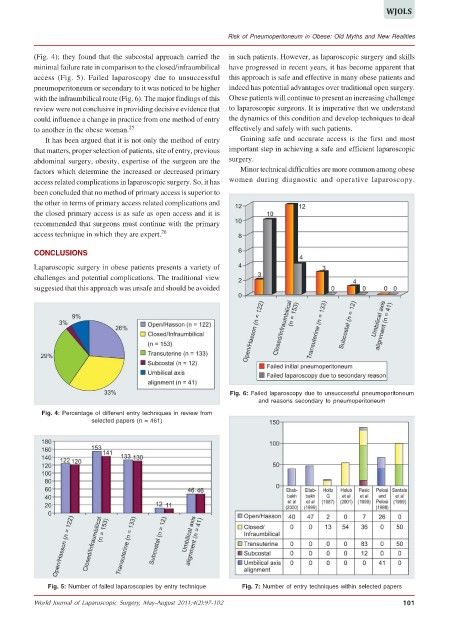
(Fig. 4); they found that the subcostal approach carried the in such patients. However, as laparoscopic surgery and skills
minimal failure rate in comparison to the closed/infraumbilical have progressed in recent years, it has become apparent that
access (Fig. 5). Failed laparoscopy due to unsuccessful this approach is safe and effective in many obese patients and
pneumoperitoneum or secondary to it was noticed to be higher indeed has potential advantages over traditional open surgery.
with the infraumbilical route (Fig. 6). The major findings of this Obese patients will continue to present an increasing challenge
review were not conclusive in providing decisive evidence that to laparoscopic surgeons. It is imperative that we understand
could influence a change in practice from one method of entry the dynamics of this condition and develop techniques to deal
to another in the obese woman. 25 effectively and safely with such patients.
It has been argued that it is not only the method of entry Gaining safe and accurate access is the first and most
that matters, proper selection of patients, site of entry, previous important step in achieving a safe and efficient laparoscopic
abdominal surgery, obesity, expertise of the surgeon are the surgery.
factors which determine the increased or decreased primary Minor technical difficulties are more common among obese
access related complications in laparoscopic surgery. So, it has women during diagnostic and operative laparoscopy.
been concluded that no method of primary access is superior to
the other in terms of primary access related complications and
the closed primary access is as safe as open access and it is
recommended that surgeons must continue with the primary
access technique in which they are expert. 26
CONCLUSIONS
Laparoscopic surgery in obese patients presents a variety of
challenges and potential complications. The traditional view
suggested that this approach was unsafe and should be avoided
Fig. 6: Failed laparoscopy due to unsuccessful pneumoperitoneum
and reasons secondary to pneumoperitoneum
Fig. 4: Percentage of different entry techniques in review from
selected papers (n = 461)
Fig. 5: Number of failed laparoscopies by entry technique Fig. 7: Number of entry techniques within selected papers
World Journal of Laparoscopic Surgery, May-August 2011;4(2):97-102 101