M.B.B.S; D.G.O; F.MAS; D.MAS;
Karad Satara Maharashtra
Introduction
Hysterectomy means removal of uterus. By open or laparoscopic way. There are many indications for hysterectomy most common are fibroid uterus, Dysfunctional uterine bleeding, uterine prolapse. Laparoscopic hysterectomy classified by Garry & Reich in to 9 types. Subtotal, supra cervical hysterectomy is type 6. First laparoscopic hysterectomy performed by Dr. Reich in 1989.
Summary of supracervical hysterectomy
For laparoscopic supracervical hysterectomy you have to take at least 3 port 4 port. after ligation of uterine pedicel and vessels by monopolar and bipolar energy sources uterus is cut from cervix. It is said that its having few advantages over total hysterectomy like maintenance of libido, in many cases patients have cyclic bleeding for 1-2 yrs after subtotal hysterectomy,no bowel/bladder complaints, no chances of vault prolapse,as anatomy of pelvis not disrupted but patient of supra cervical hysterectomy must do regular follow up to avoid cervical cancer.
CONTRAINDICATION
1- Severe COPD, cardiac diseases
2- Generalized peritonitis
3- Hypo or hyper coagulation
4- Huge broad ligament myoma
5- These are relative contraindications for laparoscopic surgeries.
PRE-OPERATION PREPARATIONS
1. Written informed consent
2. Peglac powder with a glass of water at night before surgery
3. NBM by last night before surgery.
4. Prepare parts
5. Bolus IV Antibiotics before surgery
6. Inform OT and anaesthetist
HARDWARE REQUIRED FOR SURGERY
**= Telescope 10mm 30degree,Electrosurgical unit, or ultrasonic dissector like harmonic,
**= Uterine manipulator
**= Grasper 5mm, scissors 5mm, dissectors like Maryland
**= Suture material vicryl no 1 for securing uterine vessels.
**= CO2 insufflator, Boils apparatus with ETCO2 monitoring.
Procedure of subtotal / supracervical hysterectomy
1. Shift patient to OT after all preanesthetic check up.
2. Check Camera, Light Source, CO2 Insufflator & CO2 cylinder
3. All connections of electrosurgical unit checked.
4. Patient taken on operation table,preanaesteic medications given.
5. Painting & draping done after lithotomic position.
6. SRC done.
7. General anesthesia inj. scoline given & patient intubated.
8. Surgeon is on left side of patient, assistant towards right and head end of patient. Coaxial alignment confirmed. OT Tablet ilted 0 degree down.
9. Patency of veres needle confirmed.
10. Two allis forceps applied at lower ridge of umbilicus, by 11 number blade small 2mm nick taken on skin veres needle hold like
dart & its inserted by directing towards pelvis.
11. Saline & bubble sign confirmed.
12. CO2 insufflator connected at a rate of 1litre/min and liver dullness and uniform abdominal dictation confirmed.
13. Veress needle removed incision extended up to 11 mm. Trocar inserted in perpendicular manner to skin after holding like pistol.
14. 10 mm telescope inserted light & camera joined to it, video recording started, white balancing done. CO2 tube connected & low rate increased.
15. Diagnostic laparoscopy done and target organ ia examined and two 5 & 10mm trocar inserted under illumination.
16. Uterine manipulator inserted for uterine stability & movements as per surgeons need.
17. Bipolar or harmonic in one port & semi traumatic Grasper, Maryland in other port inserted.
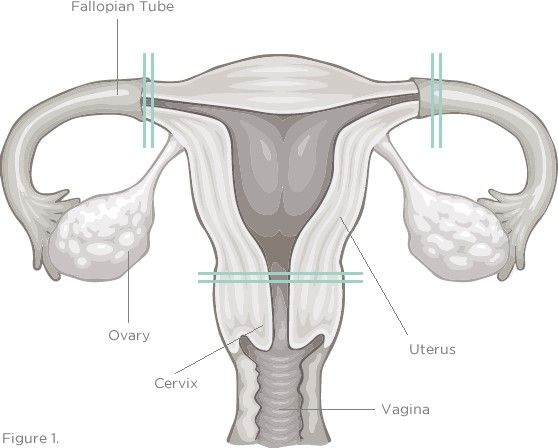
18. Round ligament at 4cm infundibulopelvic at 3cm and ovarian ligament at 2 cm cooked with bipolar forceps. If fallopian tube & ovaries to be removed remove same time otherwise they can disturb vision.
19. Now anterio & posterior folds of round ligament opened by blunt dissection.
20. Now UV fold opened with harmonic as it works on ultrasonic vibration and give bloodless dissection & bladder pushed down.
21. Posterior peritoneum 2 cm above cervical part of utero sacral ligament opened.
22. Uterine vessels secured with extracorporeal knot like mishra’s knot.
23. Now by using Bipolar, Enseal or thunderbeat uterine artery is cooked & cut and proper hemostasis assured.
24. Uterus cut from cervix by using monopolar hook.
25. Endothelium of cervix burned with energy sources.
26. Irrigation & suction done. Hemostasis confirmed.
27. Uterus taken out by morcellation..
28. 10mm ports closure done with veres needle applied suture material.
29. Dressing of the wound done.
30. Keep watch on ETCO2 level during surgery.
31. Extubate patient & shift patient to recovery room.