Prepared by: Dr. Cengiz ASCI as a project of DMAS COURSEOCTOBER 2016
Kagıthane Devlet Hastanesi Istanbul TURKEY
INTRODUCTION
- Professor Muhe of Boblingen, Germany performed the first laparoscopic cholecystectomy on September 12, 1985
- Laparoscopic cholecystectomy is the gold standard for the treatment of symptomatic gallstone disease. It is most commonly performed Minimal Access Surgery by General surgeons world wide. In this letter laparoscopic cholecystectomy technique was introduced step by step.
OPERATING ROOM DESIGN
Patient positioning
- Patient is in the supine position with a steep head-up and left tilt once the pneumoperitoneum has been established.
- Bladder deflation is not necessary
- Nasogastric tube should be inserted
Anesthesia
- Laparoscopic cholecystectomy must be performed under general anaesthesia
- cheking the all devices
- Before starting operation surgeon must be sure all devices (insufflator,camera,light source,monitor,telescope and energy devices set up) are working.
- Surgeons position
- Operation table height must be 0.49 X surgeons height
- Surgeon stands left side of the table
- Camera assistant stands left side of the surgeon
- Other assistant stands opposite side for traction of fundus
- Surgeon,target organ and monitor shold be in coaxial allignment
- Monitor should be placed 5 times far from the surgeon of its diagonal diameter and height should be 20 cm lower than surgeons eyes.
Insuflation
- One of the most important step of all laparoscopic procedures is correct and enough insuflation the abdomen with CO2.
- Evert umbilicus with two Allice clamp both side
- Make an 3 mm skin incision with no :11 blade lover or upper inner circle of umbilicus.
- Hold up the abdominal wall
- Hold the Veress needle as a dart and put on the incision
- Veress needle must be 90 degree angle to abdominal wall
- Tip of the veress needle should be inserted towards rectum
- Push the Veress needle and pass two layers of abdominal wall
- If using disposible Veress needle the indicator on top must be green
- Give 5 cc saline solution in veress needle and try to aspirate it
- Nothing must be come back
- Put the one drop saline on the Veress and hold the abdomen
- The saline must be go to abdomen
- Connect the CO2 tube.

- Alternative:If any problem with umbilicus (e.g. incision,umbilical herni) put the Veress needle on Palmers point which is located on left epigastrium andsend it towards stomach
- After reaching 10-12 mm Hg pressure take the needle out
- Enlarge the incision both side
- With an artery clamp push the rectus to lateral plan
- Insert 10 mm trocar with screwing movements slowly
- Connect the gas tube to the trochar
- Be sure your camera’s white balance is OK
- Insert the camera through the 10mm trocar
- 30 degree camera is recommended
- After entering the abdominal cavity inspect all abdomen possible bleeding, injury,adhesions or other pathologies which are undefined before.
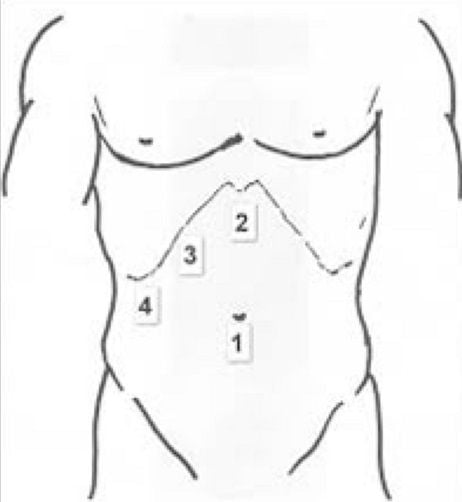
Placement of ports and instruments.
- A 1.2-cm incision is made three finger breadths below the xiphoid process and deepened into the subcutaneous fat.
- 12) An 11-mm trocar is placed into the abdominal cavity under direct vision.
- The direction of this trocar must be towards to the gallbladder through the abdominal wall, with care taken to enter just to the right of the falciform ligament.
- Operation table is then adjusted to reverse Trendelenburg position with the right side up to allow the small bowel and colon to fall away.
- A 5-mm incision on the right subcostal area and 5mm trochar is placed under direct vision .
- Another 5 mm trochar is placed 5 cm below the other 5 mm trocar.
- Two 5-mm graspers with locking mechanism is placed through each of these lateral ports.
- The lateral grasper is applied to the fundus and used to hold it cephalad over the dome of the liver.
- If gallbladder distended extremely it must be drained with a needle.Hold the Hartman’s pouch with the medial grasper and make a traction to caudolateral.
- With this maneuver straighten the cystic duct (ie, retracts it at 90° from the common bile duct [CBD]) and helps protect the CBD injury.
- Any adhesions are between the gallbladder and the omentum or duodenum must be dissected with energy devices.( momopolar, bipolar, harmonic).
- On the area of the hilum of the gallbladder it must be avoided over-dissection.
- All movement are must be controlled and towards down to up.
- After dissecting adhesions by retracting the infundibulum to the left side anterior peritoneoum of gallbladder must be dissected at the level of Hartmans pouch.
- Then by retracting the infundibulum to the right side dissect the posterior peritoneum.
- After opening both side of peritoneum there will be a vindow behind the infundibulum.
- In this bundle there is cystic duct and artery.
- Exposure them with meticulous dissection.
- After having enough space put 3 clips to the cystic duct or ligate it with extracorporeal suture
- Then apply 2 clips to the artery.
- Cut both of them with scissor or with energy device such as harmonic
- Hold the infundibulum again.
- With monopolar hook or harmonic device start the dissection to gallbladder from hepatic surface.
- Subsequently cut both side of peritoneum .
- Make some traction to upper side.
- In tis step be careful about some aberrant bile duct or artery.
- Dissect the gallbladder towards the fundus.
- Small oozing is conrolled by fulguration.
- Try to keep perforation of bladder.
- Before the cutting last attachment of fundus look for bleeding of liver and clip area.
- If there is some clots irrigate and aspirate for better view.
Mobilization and removal of gallbladder
- With 5-mm graspers are applied to the gallbladder and used to hold it over the right upper quadrant.
- The table is returned to the neutral position.
- Bed of bladder and sub- suprahepatic spaces are irrigated and suctioned to ensure adequate hemostasis and removal of any debris or bile that may have spilled.
- Gallbladder is holded on infundibulum by jaw forceps which is inserted through subxiphoid port.
- Under direct vision the gallbladder is carried in to port.
- All of them is carried out to the skin level and take the bladder out.
- The subxiphoid port and the two 5-mm ports are removed under direct vision.
- The fascia is closed at the umbilical port.
- All of the skin incisions are closed with absorbable monofilament sutures.
It gave me a detailed information on cholecystectomy which i am about to get operated for.