Dr. Rini Nikhil
- General anesthesia is to be given.
- The patient should be given a lithotomy position and bladder drained.
- Painting and draping of abdomen and perineum to be performed
- Connect and check the monitor, CCD, camera, light source.
- Do focusing at a 10cm distance for a 10mm telescope after completing white balancing.
- Insufflator is turned on to remove air from the tubing, preset pressure is kept at 15mmHg.
- Connect and set up required instruments – bipolar/ harmonic, with the electrosurgical generator.
- Attach and verify the suction irrigation system.
- Positioning of surgical team and monitor in accordance with the hierarchy and port positions; e.g.: If left-sided ipsilateral ports are used, operating surgeon stands on the left side of the patient, camera assistant on surgeon’s right side and two assistant surgeons one on the right side and second person for holding uterine manipulator.
- Take Veress needle and check patency and spring action.
- The primary port position is decided – supraumbilical for palpable uterus (14- 18 weeks of the gravid uterus) and inferior crease of the umbilicus for normal-sized uterus (less than 14 weeks size).
- Take two Allis forceps to evert and hold the lower margin of the umbilicus
- Use No. 11 blades to place a small vertical stab wound on the skin.
- Assess the abdominal wall thickness and add 4cm to it for distance to hold the Veress needle.
- Hold the Veress needle like a dart.
- Lift the abdominal wall by its full thickness using thenar and hypothenar regions of the hand and four fingers.
- Insert the Veress needle at a 90-degree angle to the lifted abdominal wall and 45-degree to the body of the patient, tip pointing towards the anus.
- Proceed with insertion till two clicks are felt, maintaining 45-degree.
- Confirm correct placement of Veress needle by irrigation, aspiration, hanging drop, and plunger test.
- Connect the insufflator tubing to the Veress needle, turn on CO2, and allow flow at 1 liter per minute with a preset pressure of 12-15mmHg.
- Observe and analyze the Quadro manometric indicators
- Once the desired pneumoperitoneum is attained remove the Veress needle.
- Extend the skin incision to 11mm horizontally; if required, by marking the circumference of the 10mm cannula at the port site.
- Hold 10mm port by the right technique like a pistol, insert it perpendicular to the inflated abdominal wall by gentle screwing movements from the elbow level and tilting it towards the pelvis when there is loss of resistance.
- Confirm intra-abdominal placing of the port by the hissing sound of air escaping through the eye of the trocar.
- Increase the flow rate of insufflation to 6litre/minute after connecting the gas tubing to the primary port.
- Insert telescope, inspect entry point, rule out any bowel or vessel injury and perform diagnostic laparoscopy.
- Keep the camera cable at 6 O’clock and the light cable at 12 O’clock positions.
- Convert the table position to 30-degree Trendelenburg.
- Place the lateral ports following the baseball diamond concept, cutting along Langer lines and inserting perpendicular to the abdominal wall.
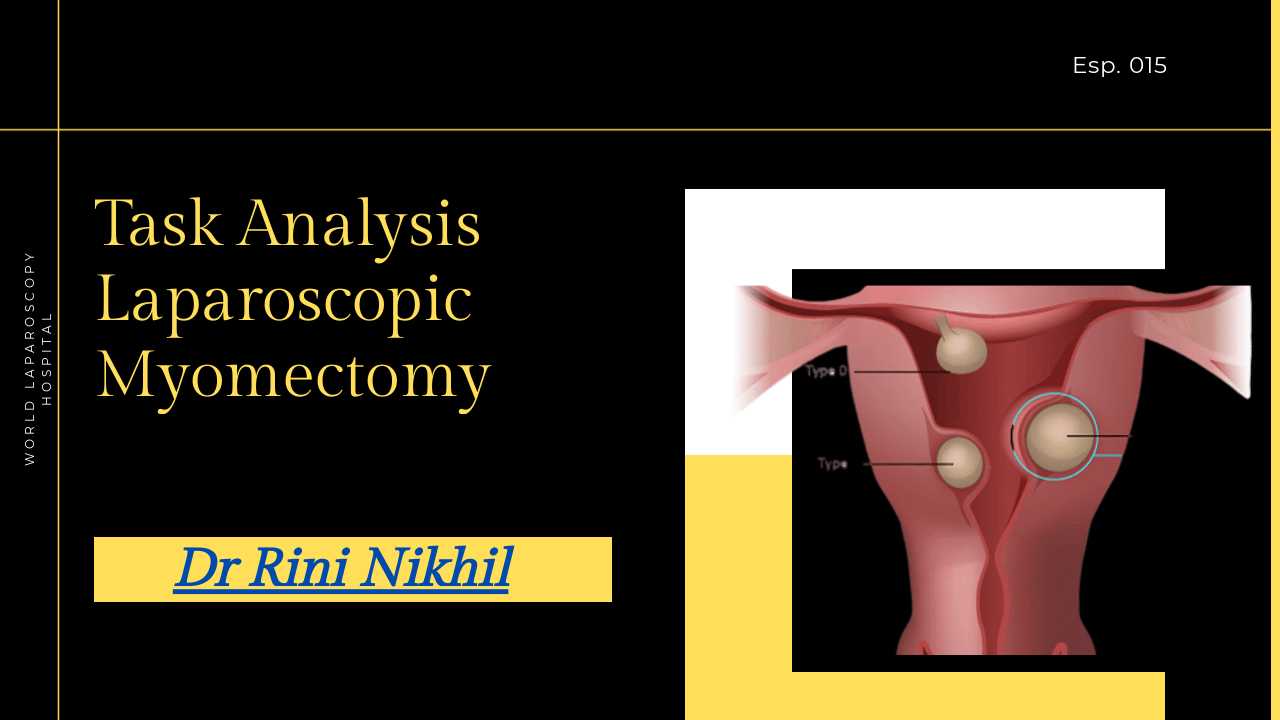
- Assess the relation of fibroid with the uterus and other pelvic structures.
- Dilute 5ml (5IU per ml) Vasopressin in 100ml saline and inject it at the maximum prominent part of the uterus, into the myometrium using an aspiration needle.
- Look for blebbing and pallor on fibroid with vasopressin injection.
- Perform hysterotomy by an oblique or sagittal incision through the serosa and myometrium of the fundus, using a Harmonic scalpel or low voltage monopolar cutting current, avoiding the cornual region and fallopian tubes.
- Open the myometrium using a harmonic scalpel, myoma screw, and myoma rod till a plane of dissection is obtained.
- Enucleate the myoma by manipulating it using a myoma screw each time inserted it towards the base of the myoma in the incision than the center of the visualized myoma for better traction.
- Use harmonic scalpel or monopolar cutting in the other hand for aiding dissection, without avulsing but carefully cutting to avoid bleeding.
- Repair the endometrial cavity using continuous No 1 Vicryl sutures through the basal layer and minimal myometrial tissue, without entering the endometrial cavity.
- Close the inner myometrium by continuous suturing with No: 2-0 Vicryl (50cm) or Barbed sutures completely obliterating the dead space to avoid hematoma formation.
- Close the outer myometrium and serosa by baseball or continuous suturing with No: 1 Vicryl or absorbable violet Braided Suture (returning with the same suture material)
- Terminate by surgeon’s knot with the tail of inner layer suture.
- Convert one of the ports, preferably closer to the pelvis, into 15mm.
- Check and insert the morcellator through the 15mm port.
- Proceed with morcellation by holding the myoma by tenaculum, feeding it to the motorized morcellator, taking care not to move the morcellator towards the tissue, instead, keeping the tissue being morcellated away from the abdominal viscera to avoid injury.
- Do irrigation and aspiration, confirm hemostasis, and proceed with port closure.
- Do closure of 15mm port used for morcellation with No-1 Vicryl using laparoscopic Cobbler needle, the cannula of Veress needle or suture passer, under visualization and avoiding tension on the sutures.
- Remove the instruments and the other ports except for the one for the telescope.
- Deflate the abdomen completely keeping the telescope inside, remove the cannula, And then the telescope.
- Close the skin incision with staplers and do dressing.
Steps 31-44: Myomectomy
Steps 45-49: Closure
Elaborated Steps:
Position the patient in the lithotomy position.
Administer general anesthesia.
Place a Foley catheter to empty the bladder.
Preoperative antibiotics are administered.
Insufflate the abdomen using CO2.
The laparoscope is inserted through a 10mm port at the umbilicus.
Place 2-3 additional trocars as required.
Identify the uterus and the location of the myoma.
Use a uterine manipulator to manipulate the uterus and improve visualization.
Dissect the round ligament and the broad ligament.
Dissect the uterine artery and vein.
Enter the uterus using a monopolar electrosurgical device.
Incise the myometrium overlying the myoma.
Use the hysteroscope to guide the dissection of the myoma.
Use a resectoscope to remove the myoma.
Coagulate the blood vessels using the monopolar electrosurgical device.
Remove the myoma in pieces or as a whole.
Use suction to clear any remaining blood clots.
Inspect the surrounding structures for any additional bleeding.
Place a drain to monitor any potential bleeding or fluid accumulation.
Close the uterine defect using an absorbable suture.
Close the serosa using an absorbable suture.
Place a haemostatic suture in the uterine artery.
Use the monopolar electrosurgical device to coagulate the suture.
Repeat the same on the other side.
Remove the uterine manipulator.
Remove the laparoscope.
Close the ports.
Deflate the abdomen.
Remove the trocars.
Close the incisions with sutures or staples.
Apply sterile dressing to the incisions.
The patient is awakened from anesthesia.
Extubate the endotracheal tube.
Move the patient to the post-anesthesia care unit.
Administer analgesics for pain management.
Monitor vital signs and urine output.
Check the dressing for bleeding or drainage.
Observe the patient for any signs of infection or complications.
Advise the patient to avoid strenuous activity for 2-4 weeks.
Advise the patient to avoid intercourse for 2-4 weeks.
Schedule a follow-up appointment.
Evaluate the patient's postoperative course.
Monitor for any complications, such as bleeding or infection.
Evaluate the patient's recovery of bowel and bladder function.
Adjust medication as needed.
Evaluate the healing of the incisions.
Monitor the patient for any signs of uterine perforation or infection.
Provide the patient with a detailed report of the procedure and postoperative care.
Advise the patient on any potential complications or side effects of the procedure.
Provide the patient with instructions on follow-up appointments and monitoring.
Advise the patient on when to resume normal activities, such as driving, work, and exercise.
The patient follows up with the surgeon at regular intervals.
The surgeon evaluates the patient's healing and progress at each follow-up appointment.
The surgeon orders any necessary imaging or laboratory tests to evaluate progress.
The surgeon adjusts medications or treatment as needed.
The surgeon monitors the patient for any signs of complications or side effects.
The surgeon communicates with the patient
Thanks for sharing.