Task Analysis Laparoscopic Bilateral Tubal Ligation By Falope Ring Application
DR. RAJANI. C. MS(OBG), DNB(OBG), FMAS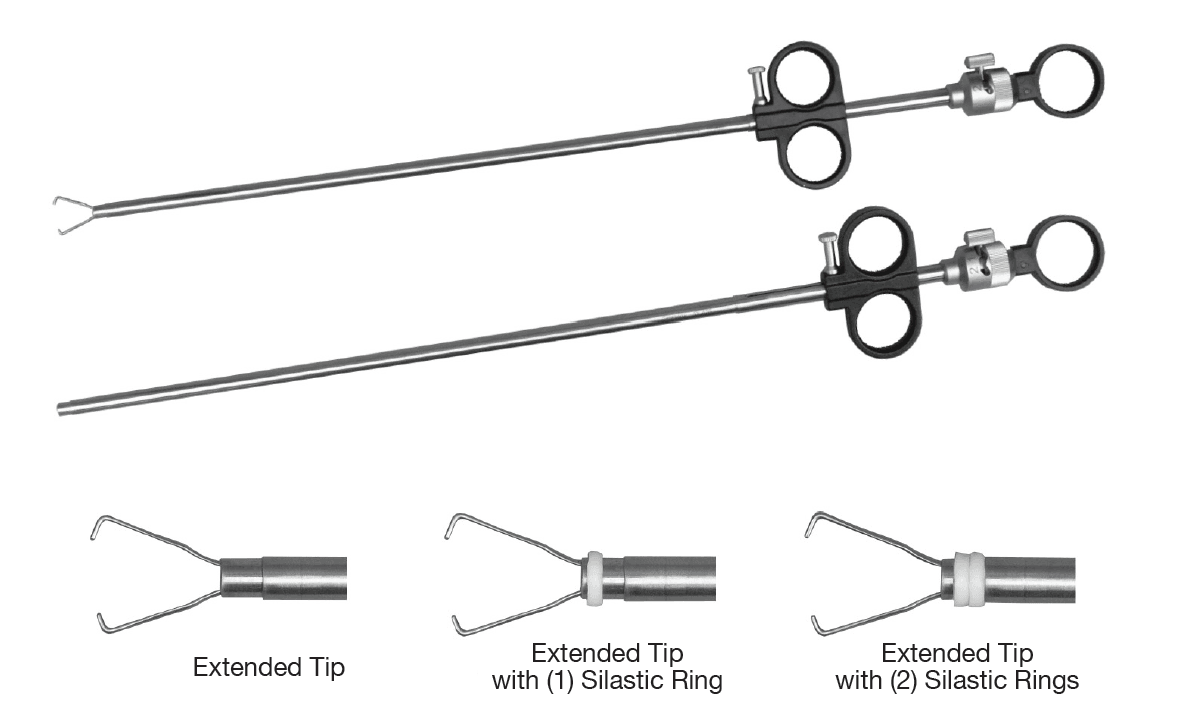
Equipment needed :
• Laparoscopic drapes, insufflators, Light source, HD camera with 30-degree telescope (10mm), seven parameter monitor, LCD monitor
• Veress needle 12 cm with 10 ml N/S syringe, and 10 ml xylocaine 2% for subcutaneous injection before doing skin incision.
• One 10 mm port and one 5 mm port
• 11 number scalpel
• Fallope ring applicator and the rings should be ready with the ring pusher. The rings should be loaded in the ring pusher not more than 10 minute before the application.
Procedure:
• Procedure can be performed under GA or LA
• Put the patient in supine position with 15-degrees head down.
• Quadrimanometric device ready, the preset pressure should not be more than 12 mm and the gas flow rate is 1L/min.
• Position of the surgical team: Surgeon on the left side of the patient and in coaxial alignment with the target organ (the tubes)and the monitor at a distant about 5*diameter of the monitor & the table height 0.49*surgeon height.
• Disinfect the abdomen from the nipple till the pubic symphysis line and to the level of anterior iliac spines laterally.
• Xylocaine 10 ml is subcutaneously infiltrated around the umbilicus
• By the use of 11 mm blade, 2 mm incision at the lower umbilical skin crease
• Verres needle is checked for valve action and patency by n/s irrigation.
• Hold it like a dart and skin thickness is elicited by holding it at the level of umbilicus and add to it 4 cm for needle tenting, needle should be perpendicular to the abdominal wall and directed toward anus, left hand should hold the lower abdominal to make it 45 degree toward patient body.
• Two clicks are heard at this time, during the rectus & peritoneum entry, then check by suction-irrigation test, hanging drop test.
• The insufflator is switched on and connected to the veress needle
• Check the flow rate and the actual pressure at this time, the flow rate not more than 1.5 L/min, the actual pressure increasing gradually, and not exceeding preset pressure.
• When the actual pressure becomes equal to the preset pressure, take out the needle, and do 10 mm smiling incision in the lower umbilical crease.
• Insert artery holding forceps to the incision to dilate the vitellointestinal duct and separate the recti muscles. (Scandanavian technique)
• Insert 10 mm umbilical port and connect the insufflator and close the valve for continuous pneumoperitoneum.
• Insert the10 mm 30-degree telescope and take a panoramic view
• 5 mm port is inserted under direct vision in the left iliac fossa 7.5 cm lateral to the umbilicus according to Baseball diamond theory.
• The fallope ring applicator is inserted through the 5 mm port under the vision of the telescope.
• Going behind the uterus, lift the tubes up
• Open the jaws of the applicator at the isthmus part of the tube 2 cm lateral to the uterus by pushing the handle
• After holding the fallopian tube with the tenaculum, verify the absence of bowel or mesosalpinx and pull the tenaculum along with the tube to make 2 cm loop
• Apply the ring for 5 seconds then release and check ring placement.
• The same is repeated on the other tube. Remove the applicator.
• Take a 5 mm telescope after white balancing and fixation before insertion through the 5mm port.
• Prepare the veress needle and make a loop of thread (proline)to use it for the closure of the 10 mm port to prevent future hernia.
• Close the umbilical 10 mm port under direct vision by no.1 vicryl.
• Deflate the abdomen gradually making jerky movement by the 5 mm telescope to avoid intestinal entrapment to the port
• Put a surgical dressing on the port sites.